Downloaded 20 times

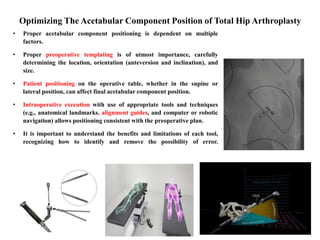
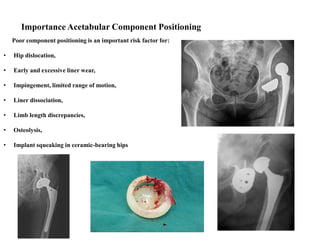
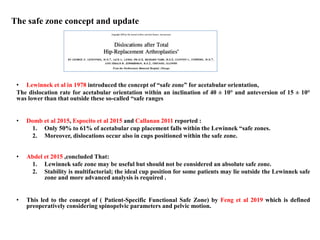


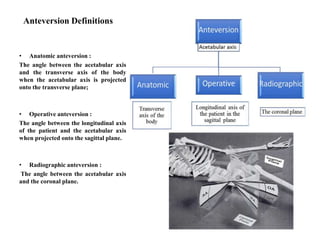



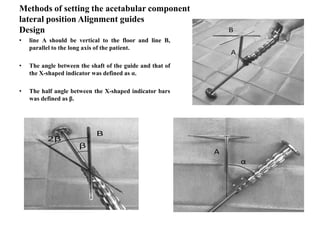
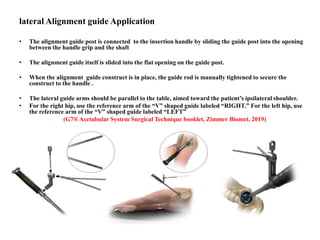



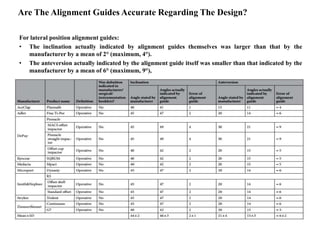








The document discusses factors that affect proper positioning of the acetabular component in total hip arthroplasty, including patient positioning, use of alignment guides, and definitions of inclination and anteversion. It finds that lateral position alignment guides indicate cup alignment based on operative definition, rather than radiographic definition, and thus are a risk factor for errors in orientation. Supine position alignment guides designed with radiographic definition do not carry the same risk of errors. Proper understanding of definitions and limitations of tools is important to minimize risk of poor component positioning.