HISTORY
1891-DR GLUCK performsfirst reported attempt at a hip
replacement with ivory.
1940-AUSTIN MOORE performs first metllaic hip replacement.
1952-AUSTIN MOORE prosthesis developed.
4.
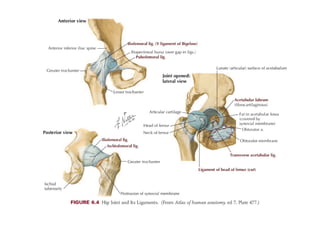
ACETABULUM-
anteverted at around15 degrees.
abdcuted 45 degrees.
divided into four quadrants.
PROXIMAL FEMUR
Femur neck anteverted 15degrees,NECK SHAFT ANGLE-
125degrees.
5.
Historically, patients 60to 75 years old were considered the
most suitable candidates for THA.
The 1994 National Institutes of Health Consensus Statement
on Total Hip Replacement concluded that “THR [total hip
replacement] is an option for nearly all patients with diseases of
the hip that cause chronic discomfort and significant functional
impairment.
In younger individuals, THA is not the only reconstruction
procedure available for a painful hip; the expanding field of hip
preservation provides surgeons with a variety of options that
may delay or obviate the need for arthroplasty.
6.
The major indicationis a medically fit patient with bilateral
severe involvement with stiffness or fixed flexion deformity
because rehabilitation may be difficult if surgery is done on one
side only.
Absolute contraindications for THA include active infec- tion of
the hip joint or any other region and any unstable medical
illnesses that would significantly increase the risk of morbidity or
mortality.
7.
Disorders of theHip Joint for Which Total Hip Arthroplasty May
Be Indicated:
Inflammatory arthritis
Rheumatoid
Juvenile idiopathic
Ankylosing spondylitis
8.
Osteoarthritis (degenerative jointdisease, hypotrophic arthritis)
Primary
Secondary
Developmental dysplasia of hip
Coxa plana (Legg-Calvé-Perthes disease) Posttraumatic
Slipped capital femoral epiphysis
Paget disease
Hemophilia
Cardiovascular complications areone of the most common
causes of perioperative mortality and hospital readmission.
Aspirin, clopidogrel, and other antiplatelet medications are best
discontinued 7 to 10 days before surgery.
If clopidogrel is to be discontinued before surgery, then it is
acceptable to continue aspirin and restart clopidogrel as soon as
the bleeding risk at the surgery site permits.
Preoperative screening for HbA1c elevation identifies patients
with poor glycemic control over a period of 2 to 3 months.
HbA1c of more than 7.5% as a significant risk factor for
postoperative joint infection.
11.
Patients having nasalcolonization with Staphylococcus aureus
are at increased risk for infection following hip arthroplasty.
Hb level in men less than 13.0 g/ dL and 12.0 g/dL for women
has been identified as an independent predictor for complications
including infection.
13.
PREOPERATIVE RADIOGRAPHS
An anteroposteriorview of the pelvis showing the proximal
femur and a lateral view of the hip and proximal femur are the
minimal views required.
The width of the medullary canal also is noted because it may
be narrow, especially in patients with dysplasia or dwarfism.
If excessive bowing or a rotational deformity is present, femoral
osteotomy may be required before or in addition to the
arthroplasty.
14.
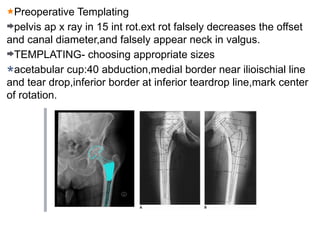
Preoperative Templating
pelvis apx ray in 15 int rot.ext rot falsely decreases the offset
and canal diameter,and falsely appear neck in valgus.
TEMPLATING- choosing appropriate sizes
acetabular cup:40 abduction,medial border near ilioischial line
and tear drop,inferior border at inferior teardrop line,mark center
of rotation.
15.
THE HIP-SPINE RELATIONSHIP
Innormal patients, the lower lumbar spine is flexible in the
sagittal plane. When moving from standing to sitting position, the
pelvis tilts posteriorly to accommodate flexion of the hip joint.
For each 1 degree of increased pelvic tilt, acetabular
anteversion increases from 0.7 to 0.8 degrees.
16.
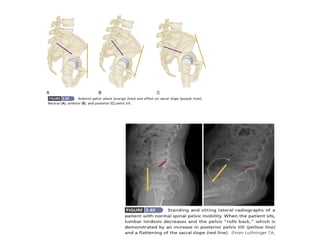
The anterior pelvicplane (APP) is defined by the points of the
two anterior superior iliac spines (ASIS) and the pubic symphysis
on a lateral radiograph of the pelvis.
Sacral slope (SS) is the angle between the superior endplate of
the S1 vertebra and a horizontal reference, typically the inferior
border of the radiograph.
Both APP and SS can be used to assess spinopel- vic motion
with changes in posture.
17.
The normal changein SS from standing to sitting is between 11
and 30 degrees. Spinopelvic stiffness is defined as a change in
SS of ≤10 degrees.
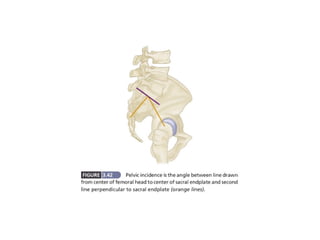
The term pelvic incidence (PI) refers to the angle between a
line drawn from the center of the femoral heads to the center of
the superior endplate of S1 and a second line drawn
perpendicular to the S1 endplate
20.
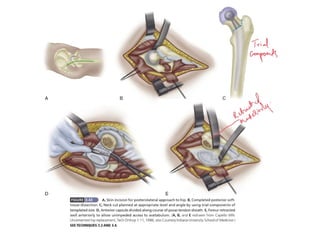
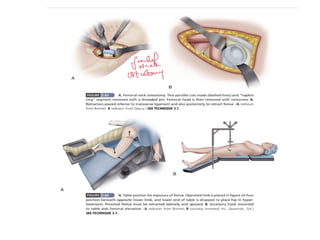
The original Charnleytechnique used the anterolateral surgical
approach with the patient supine, osteotomy of the greater
trochanter, and anterior dislocation of the hip.
The Müller technique also uses the anterolateral approach with
the patient in the lateral position but includes release of only the
anterior part of the abductor mechanism.
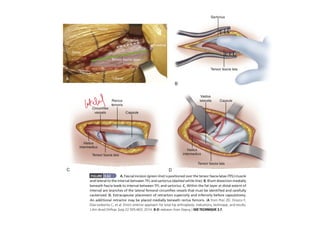
The Hardinge direct lateral approach is done with the patient
supine or in the lateral position. A muscle-splitting incision
through the gluteus medius and minimus allows anterior
dislocation of the hip and affords excellent acetabular exposure.
21.
Head et al.used a modification of the direct lateral approach, in
which the patient is in the lateral position and the vastus lateralis
is reflected anteriorly in continuity with the anterior cuff of the
abductors.
Keggi described a supine anterior approach through the medial
border of the tensor fascia lata (TFL) muscle; variations of this
approach have become popular recently and are advocated for a
reduced risk of posterior dislocation.
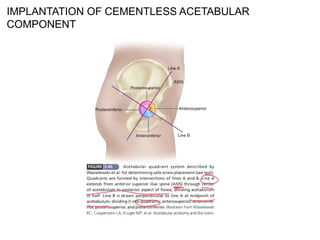
Screws placed throughthe anterosuperior quadrant emerge
within the pelvis dangerously close to the external iliac artery and
vein.
Screws passing through the anteroinferior quadrant may injure
the obturator nerve and vessels.
Screws placed through the posterosuperior and posteroinferior
quadrants do not emerge within the pelvis, but they may pass
into the sciatic notch and endanger the sciatic nerve and superior
gluteal vessels.
28.
IMPLANT FIXATION:
DORR A:<0.5intercanal diameter,cortices seen on ap an lateral
views,CEMENTLESS@femoral stemm fixation.
DORR B:0.5-0.75,posterior cortex thin on lateral
view,CEMENTLESS.
DORR C:>0.75,both cortices thin,CEMENTED.
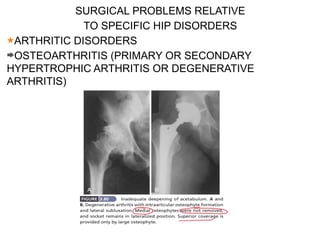
SURGICAL PROBLEMS RELATIVE
TOSPECIFIC HIP DISORDERS
ARTHRITIC DISORDERS
OSTEOARTHRITIS (PRIMARY OR SECONDARY
HYPERTROPHIC ARTHRITIS OR DEGENERATIVE
ARTHRITIS)
36.
PROTRUSIO ACETABULI
The principlesof reconstruction of a protrusion deformity are
as follows:
(1) the hip center must be placed in an anatomic location to
restore proper joint biomechanics;
(2) the intact peripheral rim of the acetabulum should be used
to support the acetabular component;
(3) the remaining cavitary and segmental defects in the medial
wall must be reconstructed, preferably with bone grafting
38.
POSTOPERATIVE
SUCTION DRAIN
IV FLUIDSAND ANTIBIOTICS
FOR first 6-8 weeks precautions to prevent dislocation.
avoiding flexion of hip beyond 90 degrees.
avoid sitting crosslegged.
avoiding internal rotation and external rotation of the hip.
avoid squatting.
39.
COMPLICATIONS
MORTALITY:30-day mortality ratewas 0.3% for primary THA
and the 90 day rate was 0.65%.
HEMATOMA FORMATION-
Common sources of bleeding are
(1) branches of the obturator vessels near the ligamentum
teres, transverse acetabular ligament, and inferior acetabular
osteophytes,
(2) the first perforating branch of the profunda femoris deep to
the gluteus maximus insertion
(3) branches of the femoral vessels near the anterior capsule,
4) branches of the inferior and superior gluteal vessels.
40.
HETEROTOPIC OSSIFICATION:Calcification canbe seen
radiographically by the third or fourth week;
The classification of Brooker et al. is useful in describing the
extent of bone formation:
Grade I: islands of bone within soft tissues
Grade II: bone spurs from the proximal femur or pelvis with at
least 1 cm between opposing bone surfaces
Grade III: bone spurs from the proximal femur or pelvis with
less than 1 cm between opposing bone surfaces
Grade IV: ankylosis

![Historically, patients 60 to 75 years old were considered the
most suitable candidates for THA.
The 1994 National Institutes of Health Consensus Statement
on Total Hip Replacement concluded that “THR [total hip
replacement] is an option for nearly all patients with diseases of
the hip that cause chronic discomfort and significant functional
impairment.
In younger individuals, THA is not the only reconstruction
procedure available for a painful hip; the expanding field of hip
preservation provides surgeons with a variety of options that
may delay or obviate the need for arthroplasty.](https://image.slidesharecdn.com/thr-250430153057-facdfd0e/85/Total-hip-ARTHROPLASTY-basic-principles-and-skills-5-320.jpg)