Downloaded 31 times
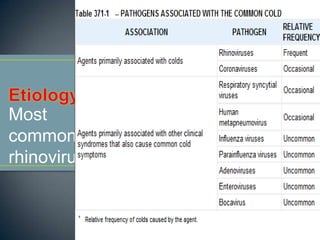

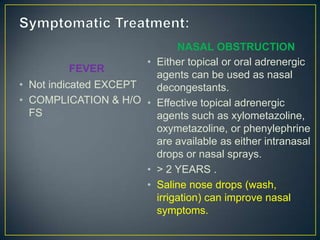

The common cold is caused by a viral infection that results in prominent nasal symptoms like rhinorrhea and congestion along with mild systemic symptoms. It is self-limited, usually lasting 1 week. Children experience 6-8 colds per year on average. Symptomatic treatment includes nasal decongestants, analgesics, and increasing fluid intake. Antibiotics are ineffective as colds are viral in nature. Complications can include sinusitis, otitis media, or asthma exacerbations.