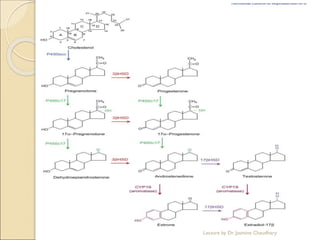
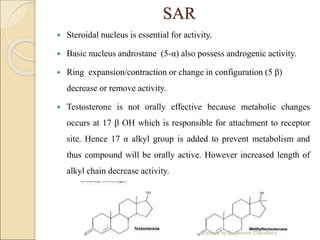
Testosterone is the main androgen hormone produced primarily in the testes and adrenal cortex. Its secretion is controlled by two hormones - FSH and LH - released by the pituitary gland in response to hypothalamic signals. FSH stimulates Sertoli cells for sperm development while LH stimulates Leydig cells to secrete testosterone. Testosterone promotes male sex characteristics and muscle building. It is metabolized in the liver but derivatives with alkyl groups at C17 are orally active. Testosterone deficiency can cause low libido, erectile dysfunction and infertility while its pharmacological uses include treatment of low testosterone conditions and for muscle building.