









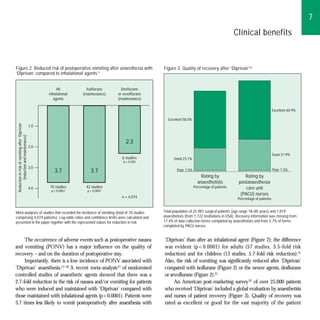





























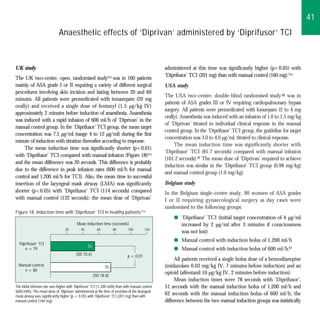

























This document discusses the clinical benefits of Diprivan (propofol). It notes that Diprivan provides: 1) Smooth, rapid induction of anesthesia within 30-60 seconds. 2) Easy control and maintenance of anesthesia at infusion rates of 4-12 mg/kg/h. 3) Prompt, clear-headed recovery with rapid return of cognitive and motor function. Recovery from Diprivan anesthesia is characterized by a low risk of postoperative nausea and vomiting compared to inhalational agents. Overall, Diprivan provides good quality induction, maintenance, and recovery from anesthesia.