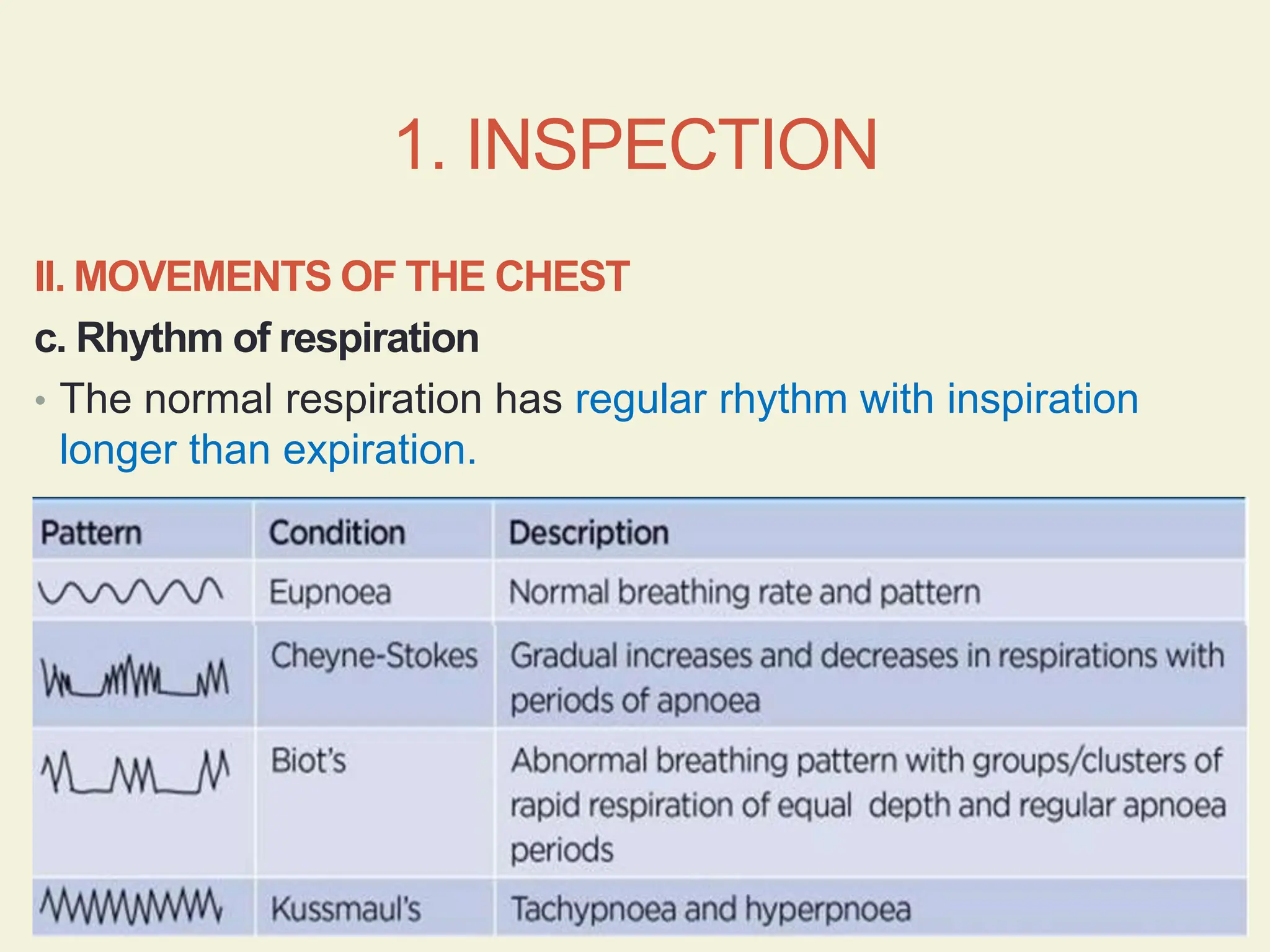
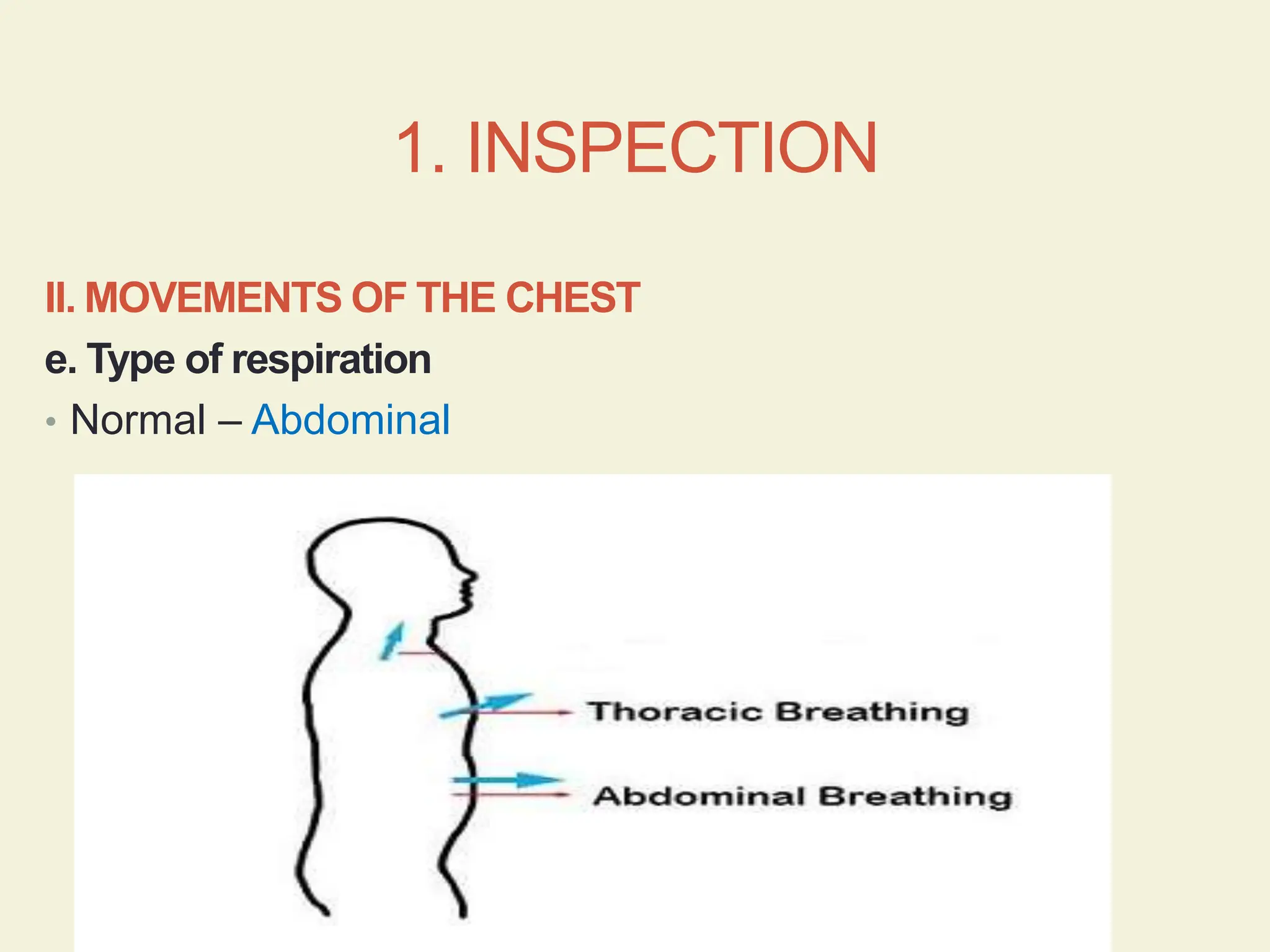
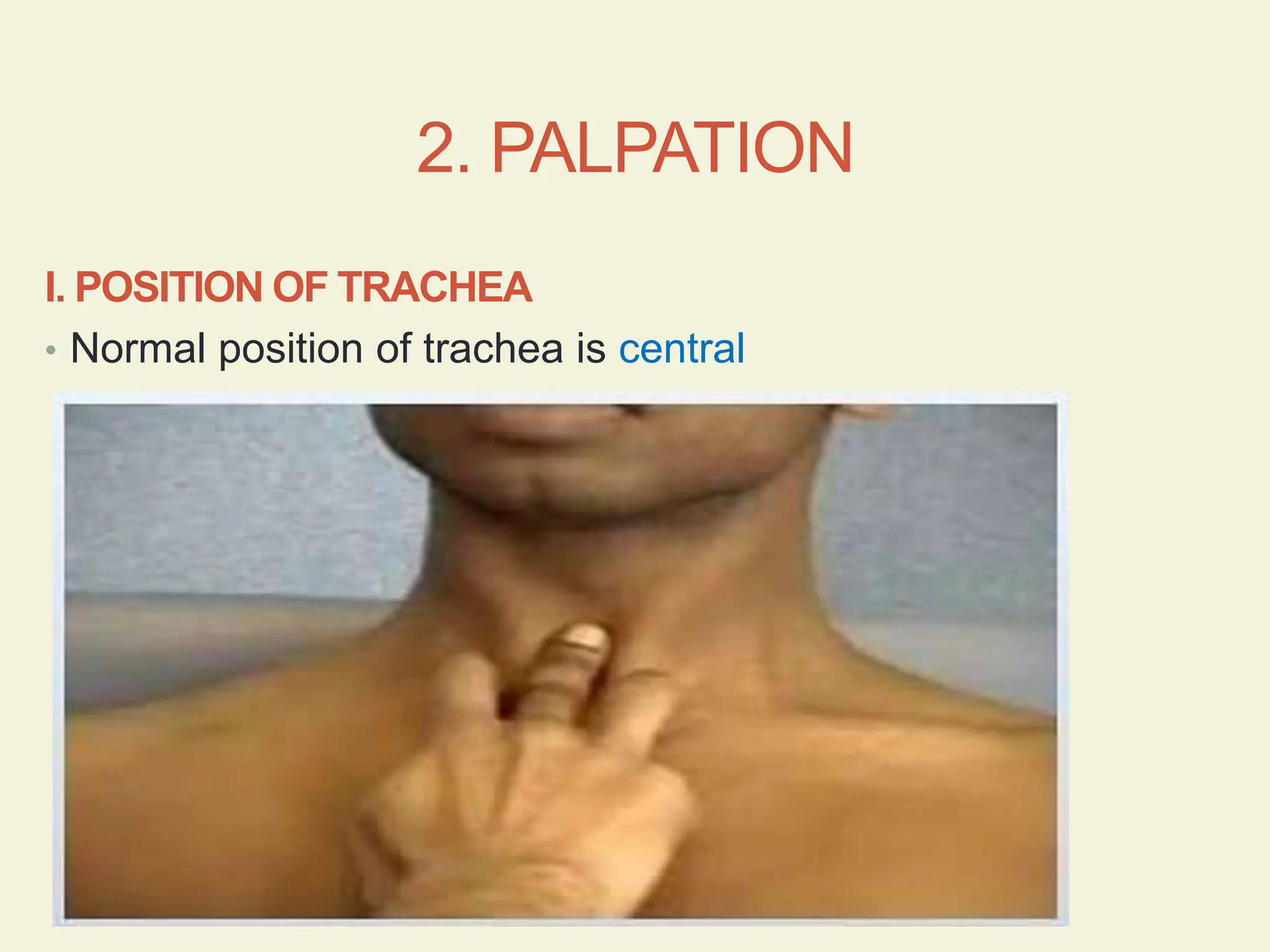
The document outlines a comprehensive procedure for the respiratory system examination, including inspection, palpation, percussion, and auscultation techniques. It details how to assess the shape, movements, and sounds of the chest, as well as specific abnormal conditions that may be observed. Key points include the normal respiratory rates, identification of respiratory patterns, and the significance of different breath sounds.













































































![Respiratory System PE-1 [Autosaved].ppttiteciex](https://cdn.slidesharecdn.com/ss_thumbnails/respiratorysystempe-1autosaved-250113170401-72d39633-thumbnail.jpg?width=640&height=640&fit=bounds)









































