Download as PPSX, PPTX
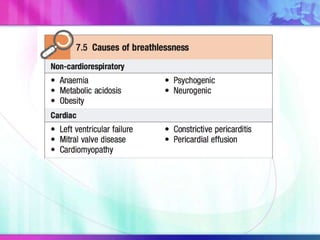
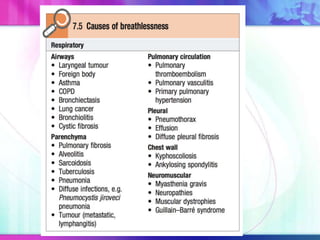
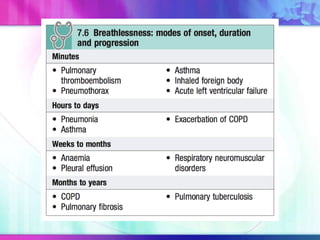
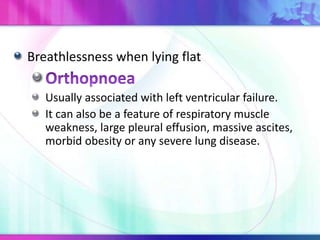
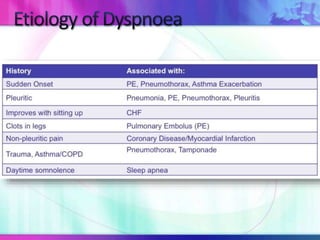
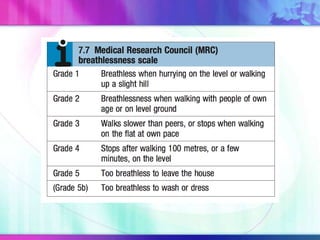
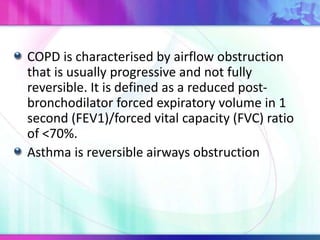

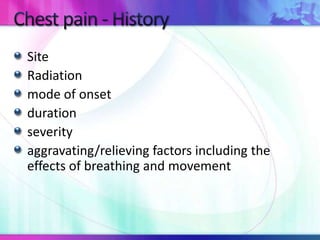
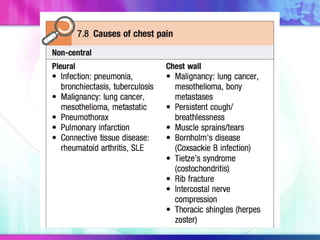

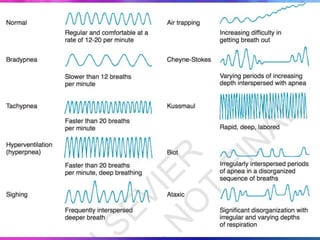





Dr. Saneesh P J discusses various symptoms of acute shortness of breath including cough, sputum production, hemoptysis, chest pain, breathlessness, and wheeze. He examines the location, quality, timing, and aggravating/relieving factors of each symptom. Dr. Saneesh also evaluates different breathing patterns, histories of underlying lung conditions, and how activity impacts shortness of breath. Based on the symptom details, potential conditions like asthma, COPD, pulmonary embolism, and heart failure are considered.












































































