The document is a detailed guide on conducting a physical examination, emphasizing the importance of environment, patient positioning, and clear communication. It outlines the main steps of physical examination, including inspection, palpation, percussion, and auscultation, while covering aspects of general appearance, vital signs, and specific systems like respiratory and cardiovascular. The document also describes techniques to assess respiratory function, identify abnormalities, and interpret findings during examination.






























































![chapter 4 Physical diagnosis [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/physicaldiagnosisautosaved-250416123318-d2df54aa-thumbnail.jpg?width=640&height=640&fit=bounds)





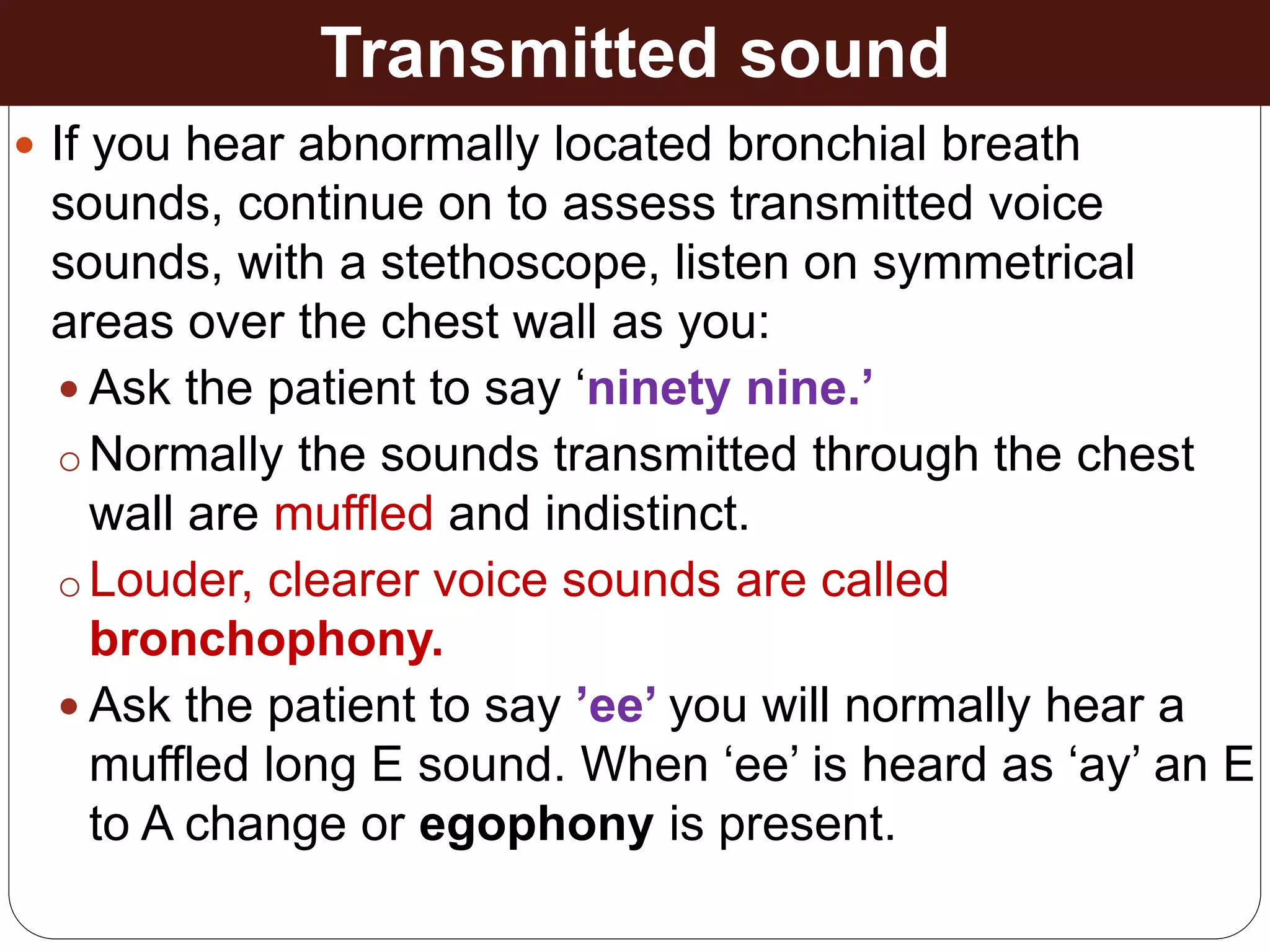
![Respiratory System PE-1 [Autosaved].ppttiteciex](https://cdn.slidesharecdn.com/ss_thumbnails/respiratorysystempe-1autosaved-250113170401-72d39633-thumbnail.jpg?width=640&height=640&fit=bounds)













































