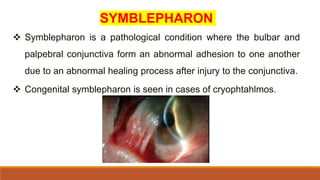
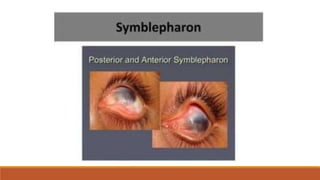
Symblepharon is a pathological condition characterized by adhesions between the eyelid and eyeball, which can be congenital or acquired due to inflammatory or traumatic etiologies. It manifests in various forms including anterior, posterior, and total symblepharon, leading to symptoms such as eye redness, burning, tearing, and restricted movement. Treatment often involves managing underlying conditions, surgical intervention, and preventing recurrence, with varying prognoses depending on severity and etiology.






























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)










