Downloaded 39 times

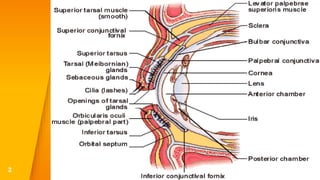
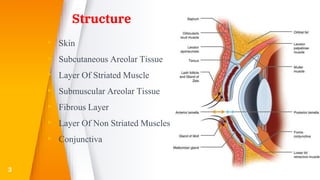
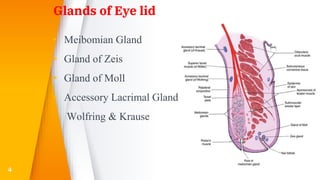
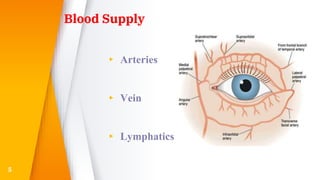
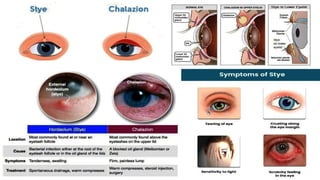
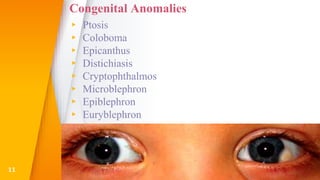
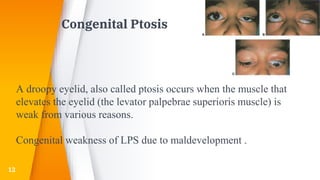

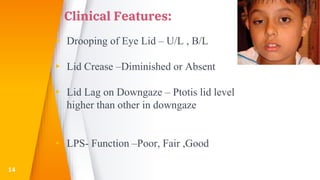
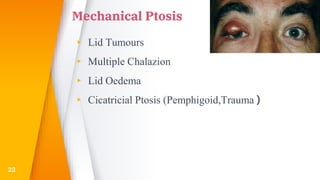


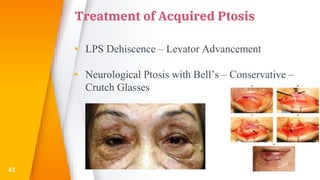
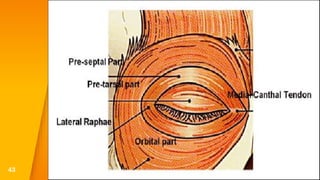
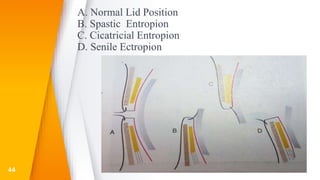
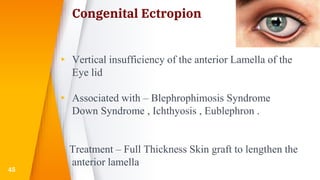
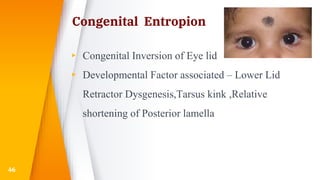
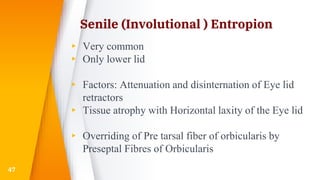
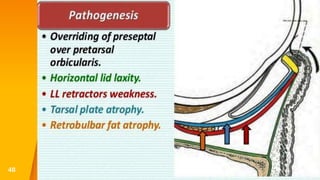

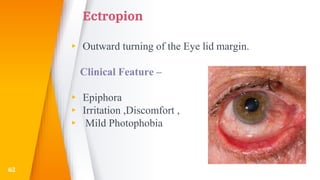
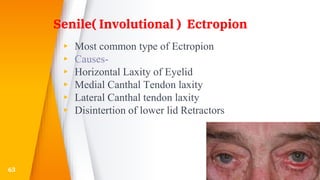
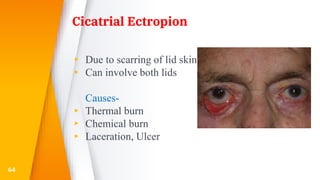
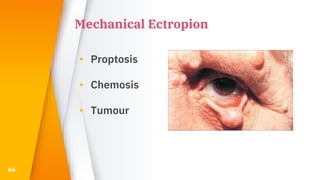
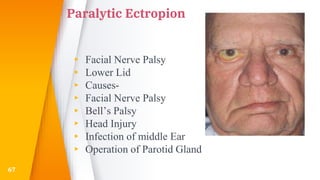
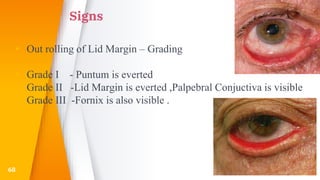
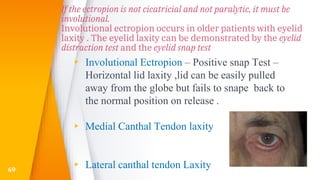
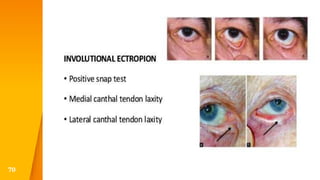

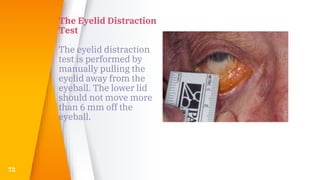

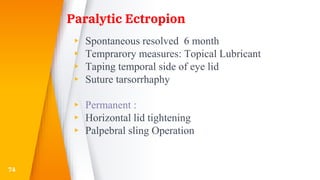
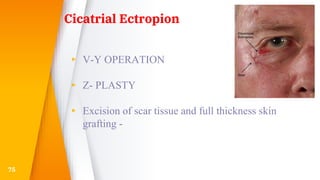











This document discusses the anatomy, structure, glands, blood supply, nerve supply, anomalies, diseases, and clinical features of the eyelid. It focuses on congenital and acquired ptosis, including the causes, clinical features, investigations, and treatment options. Specific conditions covered include congenital ptosis, neurogenic ptosis, myogenic ptosis, aponeurotic ptosis, mechanical ptosis, entropion, and ectropion. Surgical correction techniques are described for various types of ptosis and eyelid positioning anomalies.







































![CLINICAL EVALUATION AND MANAGEMENT OPTION OF AQUIRED PTOSIS [Autosaved]_09133...](https://cdn.slidesharecdn.com/ss_thumbnails/clinicalevaluationandmanagementoptionofaquiredptosisautosaved091336-250701164538-7d28272b-thumbnail.jpg?width=640&height=640&fit=bounds)















































