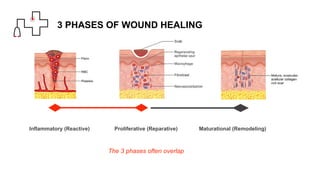
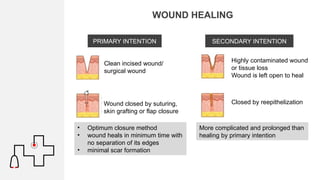
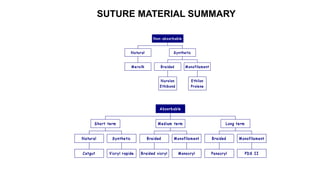
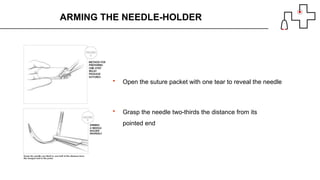
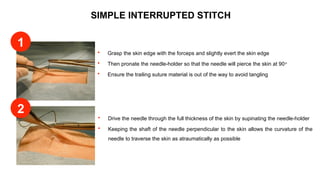
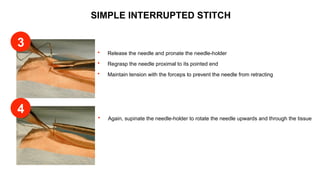
The document outlines basic surgical skills related to wound healing and suturing techniques, including types of wound healing (primary, secondary, and delayed primary closure) and various suture materials. It details the properties and handling of sutures, types of needles, and proper techniques for suturing, including the simple interrupted stitch and suture removal guidelines. Additionally, it emphasizes the importance of selecting appropriate suturing methods and materials based on wound type and tissue characteristics.