This document provides an overview of ocular motility disorders, including:
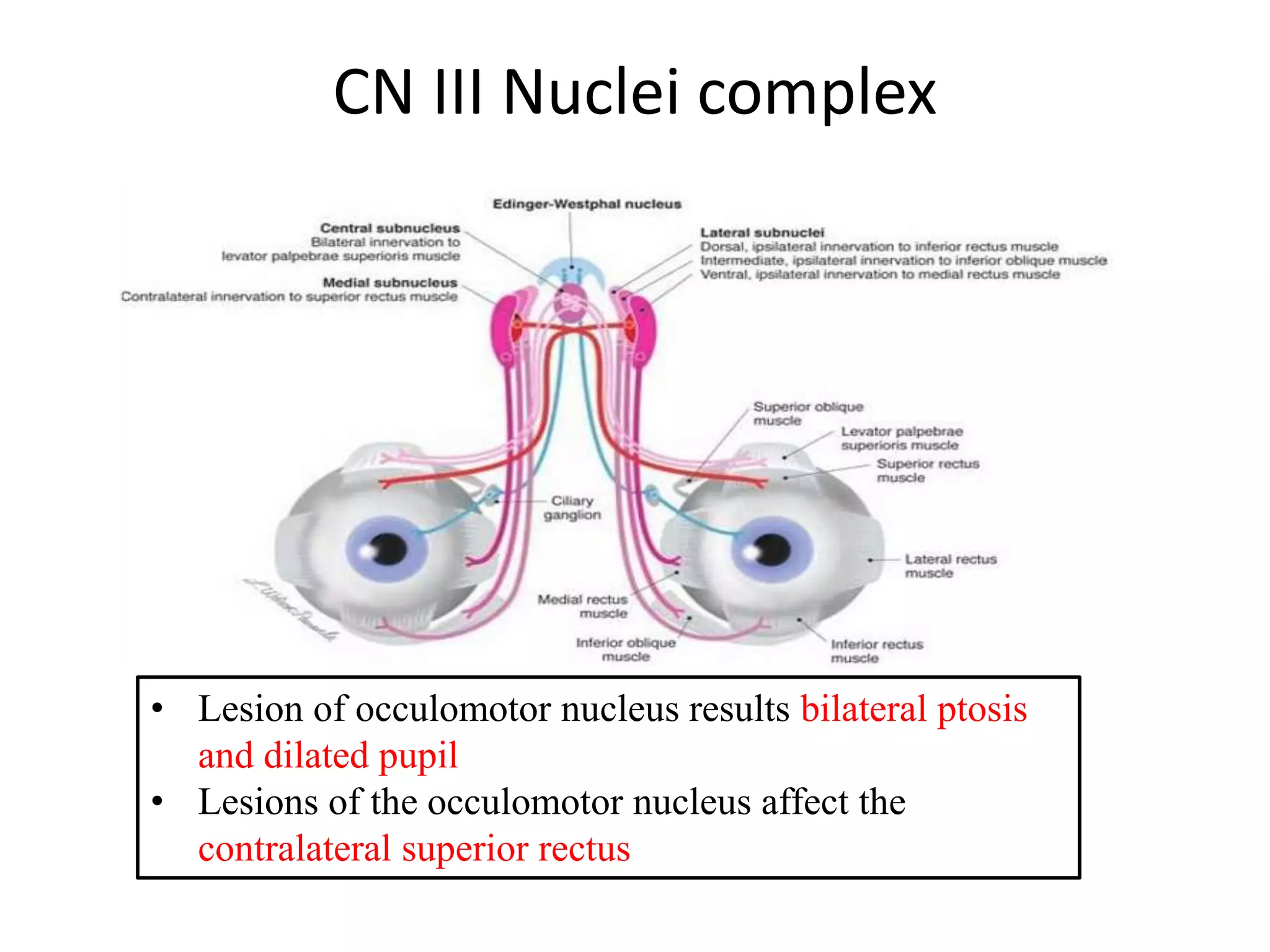
1. The anatomy and function of the extraocular muscles and neural control centers.
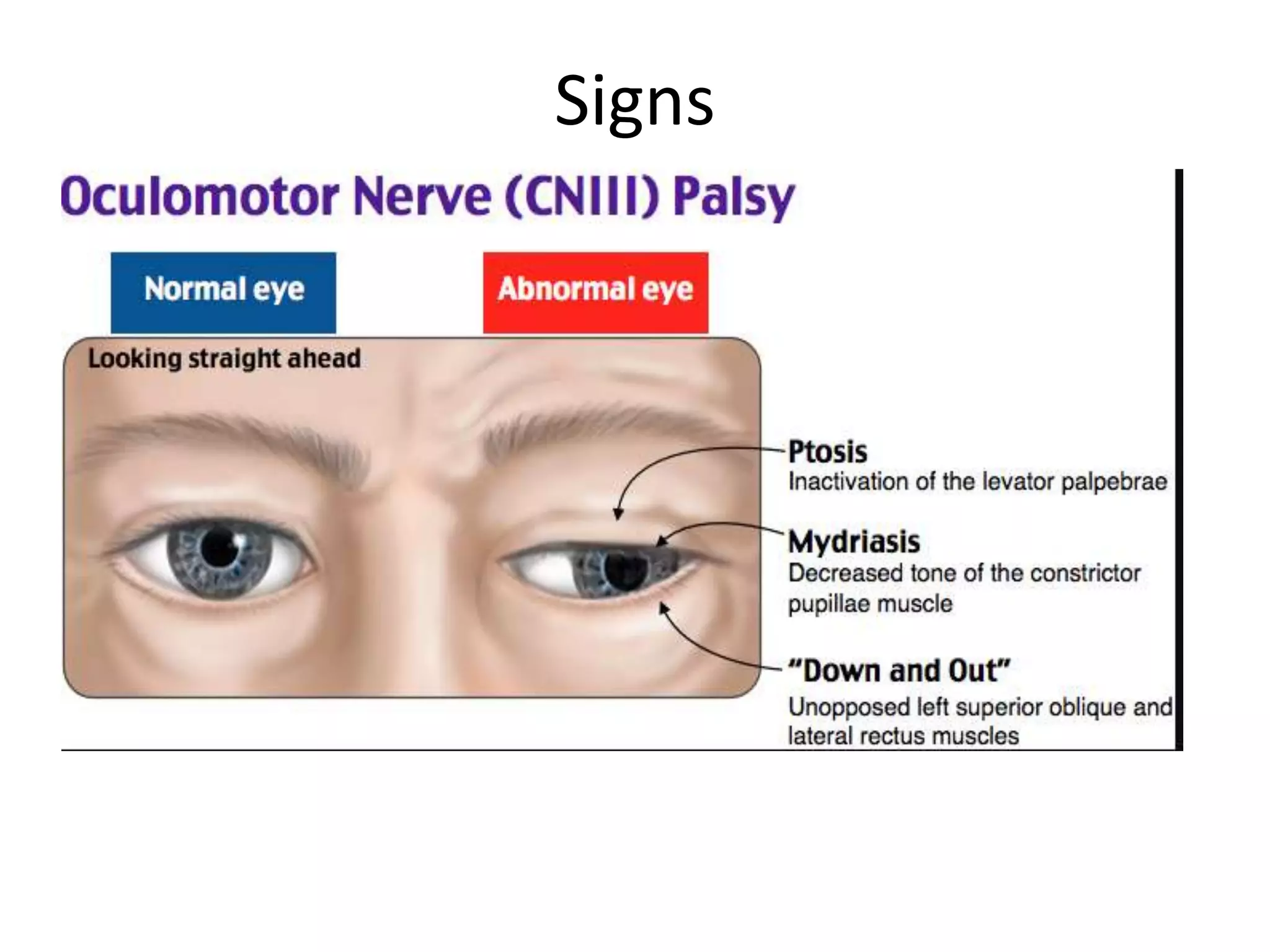
2. Classification of abnormal eye movements including types (e.g. saccades, smooth pursuit) and causes (e.g. myopathies, nerve palsies).
3. Specific disorders are described in detail such as internuclear ophthalmoplegia, Parinaud's syndrome, and progressive supranuclear palsy.
4. Nystagmus is classified and mechanisms are discussed.