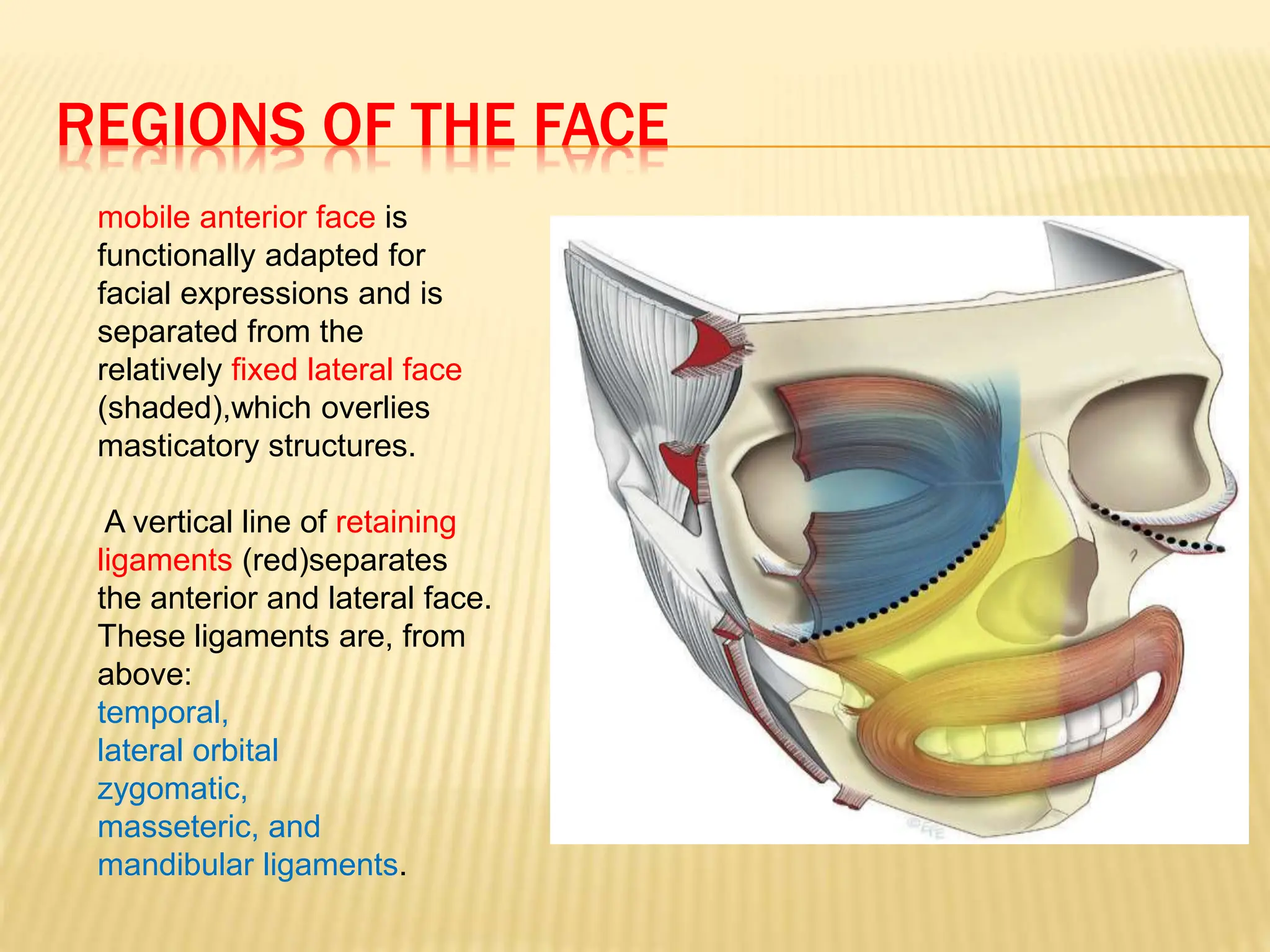
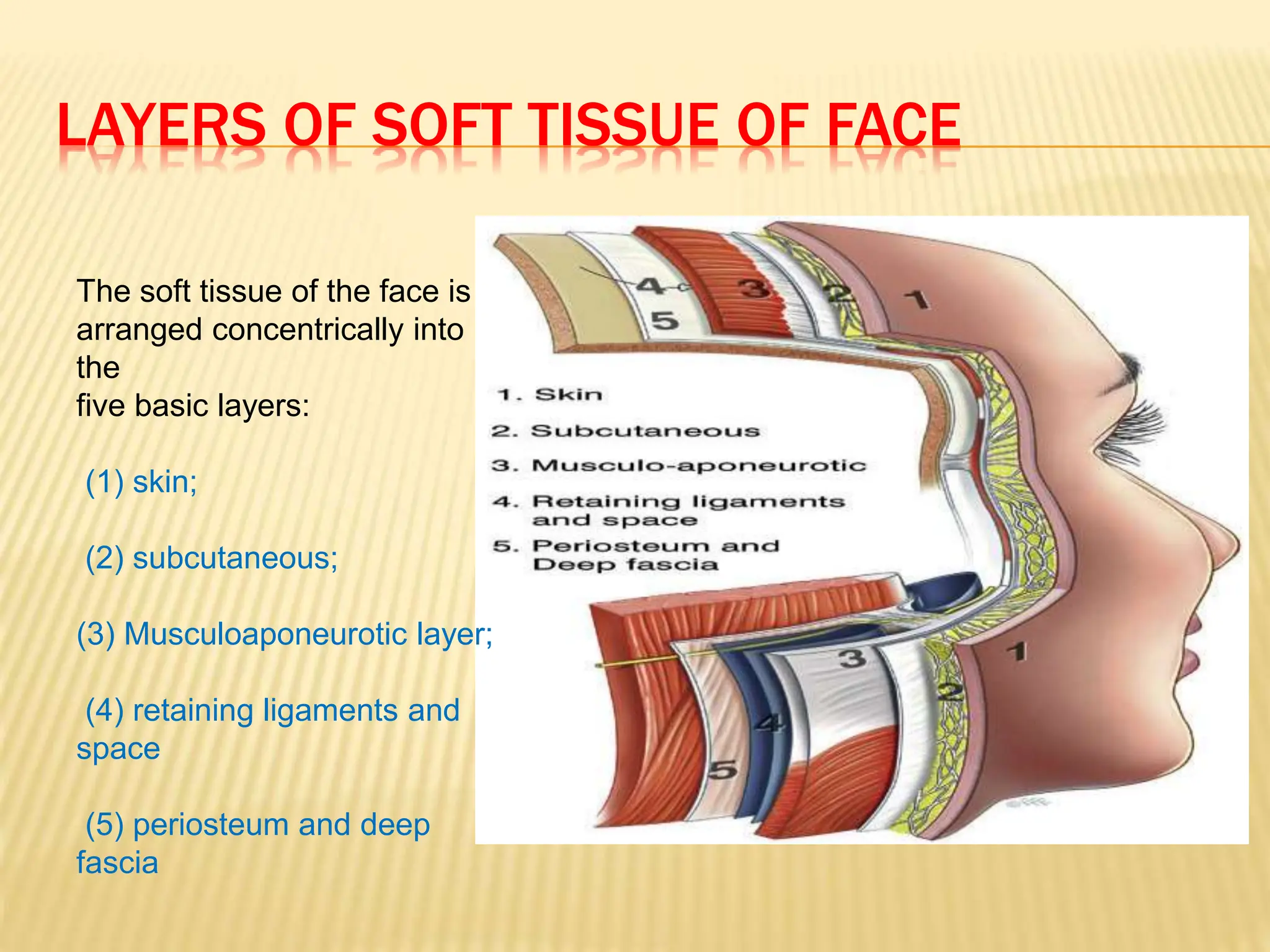
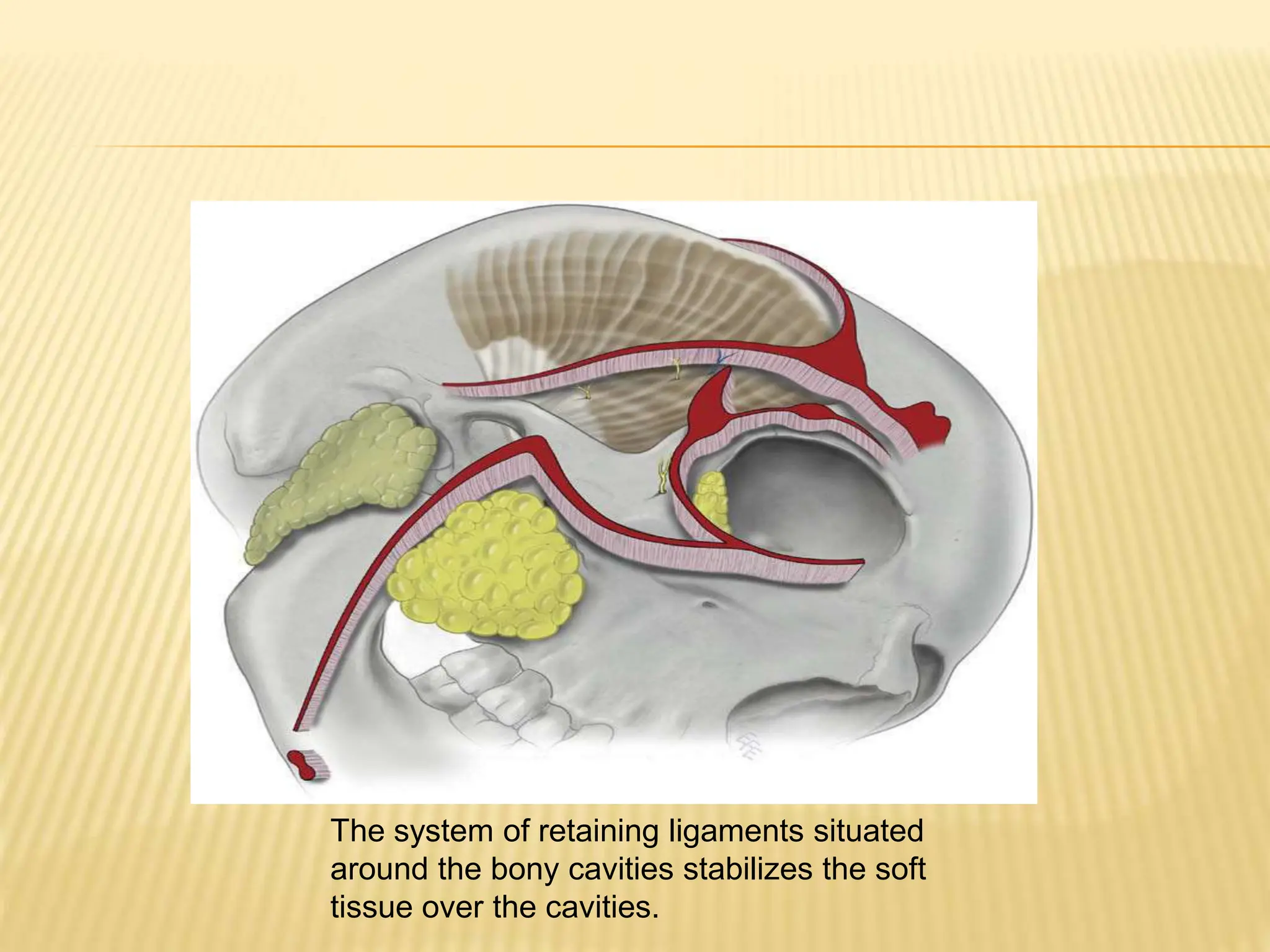
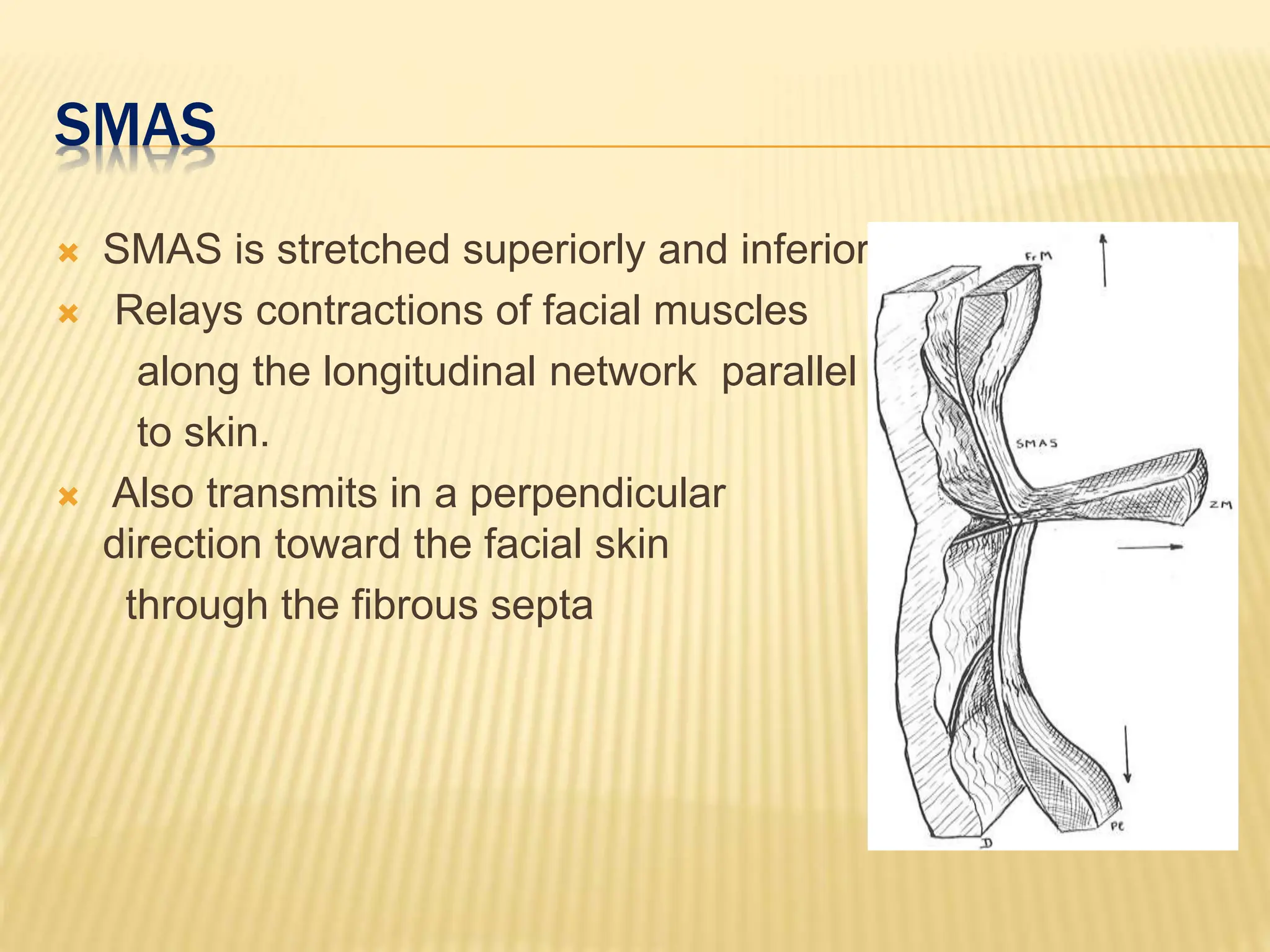
This document discusses the anatomy of the aging face. It describes the five layers of soft tissue in the face - skin, subcutaneous layer, musculoaponeurotic layer, retaining ligaments/spaces, and periosteum/deep fascia. It highlights how aging affects these layers and the spaces between them. Specifically, it notes how the retaining ligaments weaken with age, allowing the spaces to expand and bulge out more, contributing to signs of aging like jowls, malar bags, and labiomandibular folds. The document provides a detailed overview of facial anatomy and changes that occur with aging.