Downloaded 121 times













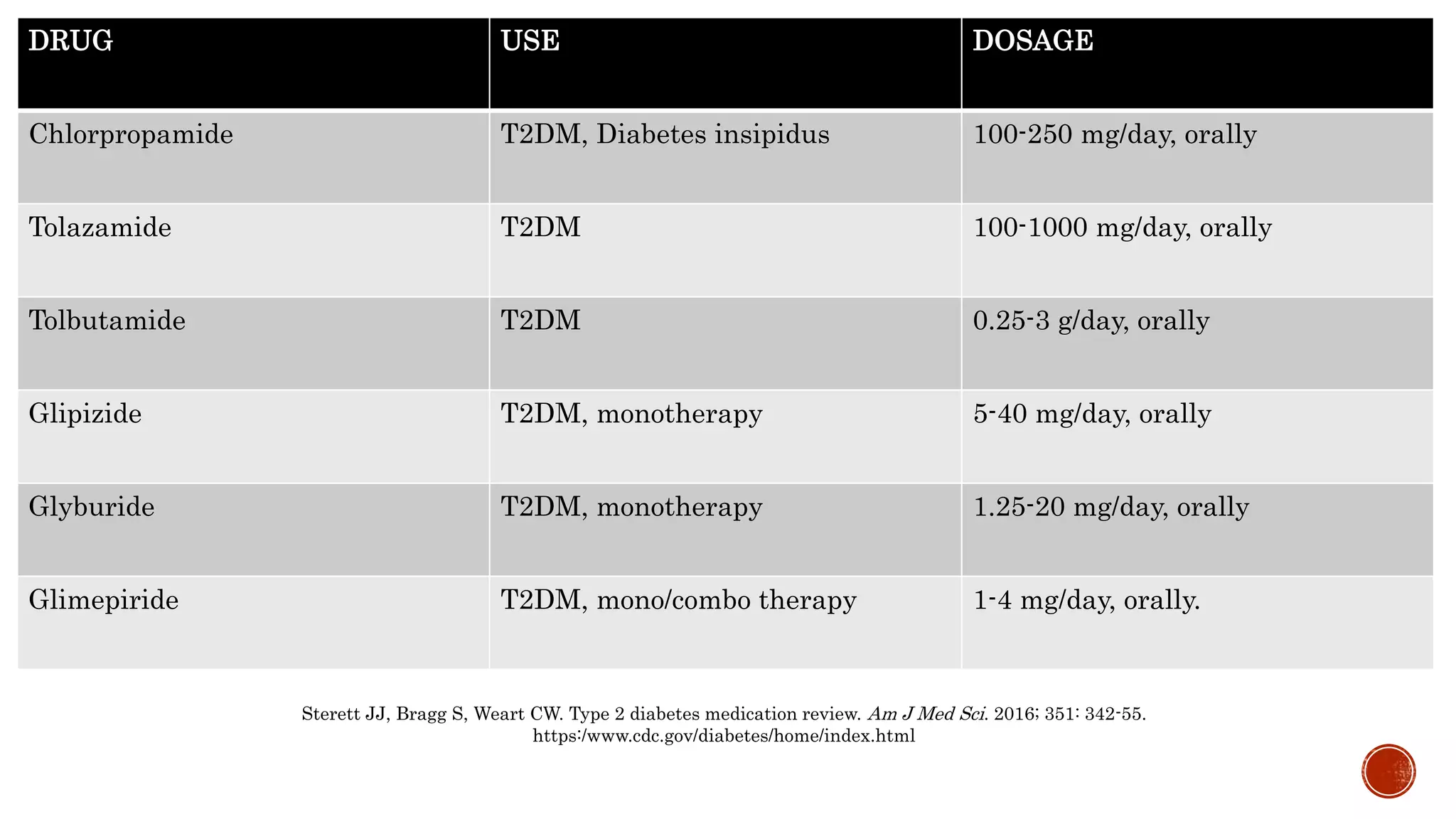







The document discusses sulfonylureas, a class of antidiabetic drugs that stimulate insulin secretion and are primarily used for managing type 2 diabetes, especially when pancreatic beta-cell function is sufficient. It details the mechanism of action, pharmacokinetic profiles, therapeutic efficacy, potential side effects, and interactions with other drugs, emphasizing caution in patients with specific conditions. It also provides guidelines on usage and highlights that first-generation sulfonylureas are less commonly used due to higher risks of adverse effects.























































































