Classification of Diabetesmellitus
There are two main types of diabetes
Type 1 (requiring insulin for survival) and
Type 2 (may or may not require insulin for
metabolic control)
It is recommended that the terms
Insulin-dependent diabetes mellitus (IDDM)
for type 1 and
Non-insulin-dependent diabetes mellitus
(NIDDM)for type 2
No longer be used
3.
Antidiabetic Drugs
Antidiabeticdrug includes insulin & oral hypoglycemic agents
Insulin
Can be commercially prepared for treatment of type I, gestational &
some type II diabetes
The first insulin which was made available commercially for clinical use
was amorphous insulin
Purification of amorphous insulin led to crystalline insulin
Which is now commonly called regular insulin
Insulin injection, USP, is made from zinc insulin crystal
Sometimes regular insulin solutions have been prepared at a pH of
2.8 – 3.5
If the pH were increased above the acidic range, particles will be
formed
Neutral insulin solutions have greater stability than acidic solutions
Neutral solutions maintain nearly full potency when stored up to
18 months at 5o
C & 25o
C
4.
Oral hypoglycemic agents
The oral hypoglycemic agents
Are used to treat patients with type 2 diabetes that is not
controlled by diet and exercise alone
Are not effective for treating type 1 diabetes
May also be used with insulin in the management of some
patients with diabetes mellitus
Use of an oral antidiabetic drug with insulin
May decrease the insulin dosage in some individuals
The patient most likely to respond well to oral
hypoglycemic agents is one who develops diabetes after
age 40 and has had diabetes less than 5 years
Patients with long-standing disease may require a
combination of a
Hypoglycemic drug and insulin to control their
hyperglycemia
5.
Oral hypoglycemic agentscont.
Oral hypoglycemic drugs act in one or more
of the following:
Stimulating the release of insulin by the
pancreas (Insulinotropic agents )
Slowing the absorption of glucose from
the intestines
Decreasing glucose synthesis and
release by the liver
Making cells more sensitive to insulin
(e.g., muscle and liver)
6.
CURRENT DRUGS ONTHE MARKET
Drugs currently available for
treatment of hyperglycemia
associated with diabetes mellitus
fall into four classes:
Insulin and its analogs
Insulinotropic agents
Insulin-sensitizing agents
Alpha-Glucosidase inhibitors
7.
CURRENT DRUGS ONTHE MARKET cont.
Types of oral antidiabetic drugs are currently in use:
Sulfonylureas (e.g. glyburide/ Glibenclamide/,
glimepiride)
Meglitinides/Glinides (e.g. nateglinide, repaglinide)
Biguanides (e.g. metformin)
Alpha (α)-glucosidase inhibitors (e.g. acarbose,
miglitol)
Thiazolidinediones (e.g. pioglitazone, rosiglitazone)
8.
Insulinotropic agents
Insulinotropicagents are agents that directly stimulate
the release of insulin from pancreatic β-cells
The drugs in this class are often divided into the
subclasses:
Sulfonylureas and glinides
These compounds are structurally related and
share a common mechanism of action
Sulfonylureas
It appear to lower blood glucose by stimulating
the beta cells of the pancreas to release insulin
They are not effective
If the beta cells of the pancreas are unable to
release a sufficient amount of insulin to meet
the individual’s needs
9.
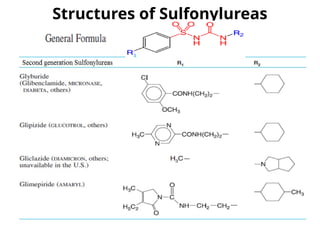
Sulfonylureas
The sulfonylureasare divided into different generations:
The first generation sulfonylureas
Includes tolbutamide, acetohexamide, tolazamide, and
chlorpropamide
Are not commonly used today because they have a
Long duration of action and
Higher incidence of adverse reactions, and
Are more likely to react with other drugs
The second generation sulfonylureas
Includes glyburide (glibenclamide), glipizide, gliclazide,
They are the more commonly used sulfonylureas
Third generation
Glimepiride
Some classify glimepiride as second-generation, while others
classify it as third-generation
Fourth generation (light-dependent)
JB253
10.
Sulfonylureas cont.
The mechanismsof action of the sulfonylureas include:
Stimulation of insulin release from the β-cells of the
pancreas
Reduction of serum glucagon levels and
Increased binding of insulin to target tissues and
receptors
They act by closing membrane-bound ATP-sensitive
potassium (KATP) channels on the β-cell
Causing depolarization and the opening of voltage-
gated calcium channels.
The resulting influx of Ca2+
triggers exocytosis of
insulin
11.
Sulfonylureas cont.
These drugsare contraindicated in patients with hepatic
or renal insufficiency
Because delayed excretion of the drug, resulting in its
accumulation, may cause hypoglycemia
The sulfonylureas traverse the placenta and can deplete
insulin from the fetal pancreas;
Therefore, type II DM pregnant women should be
treated with insulin
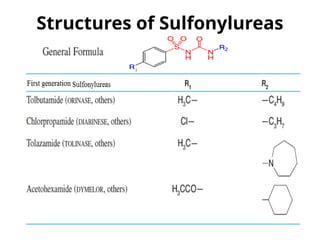
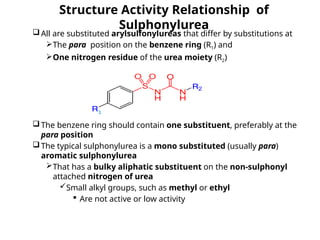
Structure Activity Relationshipof
Sulphonylurea
All are substituted arylsulfonylureas that differ by substitutions at
The para position on the benzene ring (R1) and
One nitrogen residue of the urea moiety (R2)
The benzene ring should contain one substituent, preferably at the
para position
The typical sulphonylurea is a mono substituted (usually para)
aromatic sulphonylurea
That has a bulky aliphatic substituent on the non-sulphonyl
attached nitrogen of urea
Small alkyl groups, such as methyl or ethyl
Are not active or low activity
15.
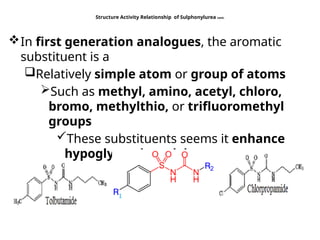
Structure Activity Relationshipof Sulphonylurea cont.
In first generation analogues, the aromatic
substituent is a
Relatively simple atom or group of atoms
Such as methyl, amino, acetyl, chloro,
bromo, methylthio, or trifluoromethyl
groups
These substituents seems it enhance
hypoglycemic activity
16.
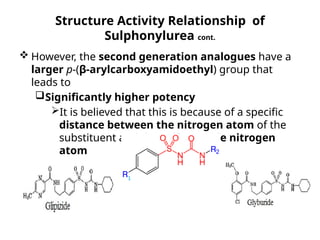
Structure Activity Relationshipof
Sulphonylurea cont.
However, the second generation analogues have a
larger p-(β-arylcarboxyamidoethyl) group that
leads to
Significantly higher potency
It is believed that this is because of a specific
distance between the nitrogen atom of the
substituent and the sulfonamide nitrogen
atom
17.
Structure Activity Relationshipof Sulphonylurea
cont.
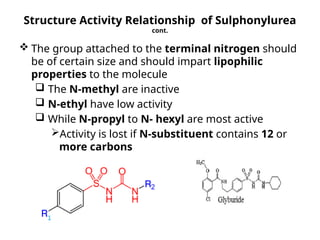
The group attached to the terminal nitrogen should
be of certain size and should impart lipophilic
properties to the molecule
The N-methyl are inactive
N-ethyl have low activity
While N-propyl to N- hexyl are most active
Activity is lost if N-substituent contains 12 or
more carbons
18.
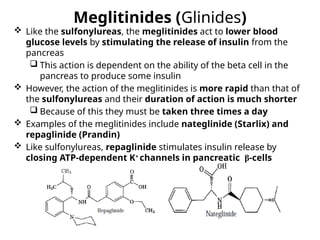
Meglitinides (Glinides)
Likethe sulfonylureas, the meglitinides act to lower blood
glucose levels by stimulating the release of insulin from the
pancreas
This action is dependent on the ability of the beta cell in the
pancreas to produce some insulin
However, the action of the meglitinides is more rapid than that of
the sulfonylureas and their duration of action is much shorter
Because of this they must be taken three times a day
Examples of the meglitinides include nateglinide (Starlix) and
repaglinide (Prandin)
Like sulfonylureas, repaglinide stimulates insulin release by
closing ATP-dependent K+
channels in pancreatic β-cells
19.
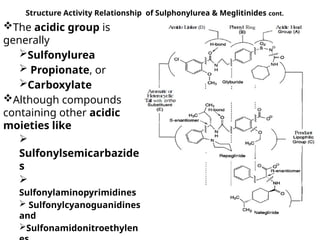
Structure Activity Relationshipof Sulphonylurea &
Meglitinides
Hypoglycemic
sulfonylureas and glinides
contain an acidic
functional group (A in Fig.)
That is required for
insulinotropic activity
In all of the marketed
drugs of this class
The acidic group is
attached to a phenyl ring
(B in Fig.)
20.
Structure Activity Relationshipof Sulphonylurea & Meglitinides cont.
The acidic group is
generally
Sulfonylurea
Propionate, or
Carboxylate
Although compounds
containing other acidic
moieties like
Sulfonylsemicarbazide
s
Sulfonylaminopyrimidines
Sulfonylcyanoguanidines
and
Sulfonamidonitroethylen
21.
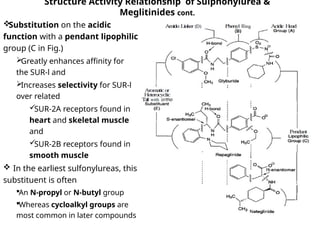
Structure Activity Relationshipof Sulphonylurea &
Meglitinides cont.
Substitution on the acidic
function with a pendant lipophilic
group (C in Fig.)
Greatly enhances affinity for
the SUR-l and
Increases selectivity for SUR-l
over related
SUR-2A receptors found in
heart and skeletal muscle
and
SUR-2B receptors found in
smooth muscle
In the earliest sulfonylureas, this
substituent is often
An N-propyl or N-butyl group
Whereas cycloalkyl groups are
most common in later compounds
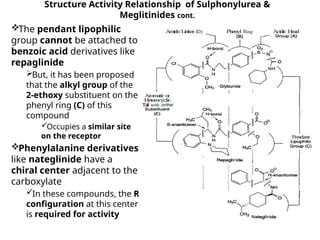
22.
Structure Activity Relationshipof Sulphonylurea &
Meglitinides cont.
The pendant lipophilic
group cannot be attached to
benzoic acid derivatives like
repaglinide
But, it has been proposed
that the alkyl group of the
2-ethoxy substituent on the
phenyl ring (C) of this
compound
Occupies a similar site
on the receptor
Phenylalanine derivatives
like nateglinide have a
chiral center adjacent to the
carboxylate
In these compounds, the R
configuration at this center
is required for activity
23.
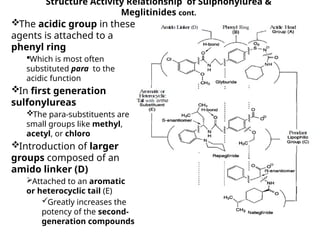
Structure Activity Relationshipof Sulphonylurea &
Meglitinides cont.
The acidic group in these
agents is attached to a
phenyl ring
Which is most often
substituted para to the
acidic function
In first generation
sulfonylureas
The para-substituents are
small groups like methyl,
acetyl, or chloro
Introduction of larger
groups composed of an
amido linker (D)
Attached to an aromatic
or heterocyclic tail (E)
Greatly increases the
potency of the second-
generation compounds
24.
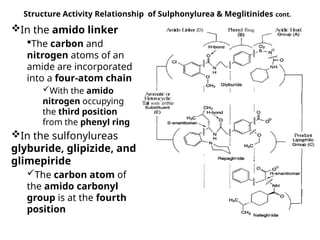
Structure Activity Relationshipof Sulphonylurea & Meglitinides cont.
In the amido linker
The carbon and
nitrogen atoms of an
amide are incorporated
into a four-atom chain
With the amido
nitrogen occupying
the third position
from the phenyl ring
In the sulfonylureas
glyburide, glipizide, and
glimepiride
The carbon atom of
the amido carbonyl
group is at the fourth
position
25.
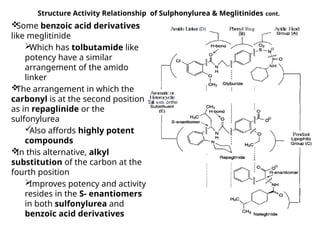
Structure Activity Relationshipof Sulphonylurea & Meglitinides cont.
Some benzoic acid derivatives
like meglitinide
Which has tolbutamide like
potency have a similar
arrangement of the amido
linker
The arrangement in which the
carbonyl is at the second position
as in repaglinide or the
sulfonylurea
Also affords highly potent
compounds
In this alternative, alkyl
substitution of the carbon at the
fourth position
Improves potency and activity
resides in the S- enantiomers
in both sulfonylurea and
benzoic acid derivatives
26.
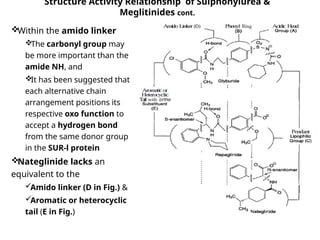
Structure Activity Relationshipof Sulphonylurea &
Meglitinides cont.
Within the amido linker
The carbonyl group may
be more important than the
amide NH, and
It has been suggested that
each alternative chain
arrangement positions its
respective oxo function to
accept a hydrogen bond
from the same donor group
in the SUR-l protein
Nateglinide lacks an
equivalent to the
Amido linker (D in Fig.) &
Aromatic or heterocyclic
tail (E in Fig.)
27.
Structure Activity Relationshipof Sulphonylurea &
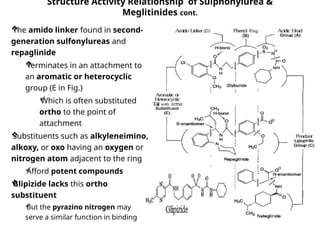
Meglitinides cont.
The amido linker found in second-
generation sulfonylureas and
repaglinide
Terminates in an attachment to
an aromatic or heterocyclic
group (E in Fig.)
Which is often substituted
ortho to the point of
attachment
Substituents such as alkyleneimino,
alkoxy, or oxo having an oxygen or
nitrogen atom adjacent to the ring
Afford potent compounds
Glipizide lacks this ortho
substituent
But the pyrazino nitrogen may
serve a similar function in binding
28.
Insulin-Sensitizing Agents
Twosubclasses of insulin-sensitizing agents are
currently available:
The biguanides and
The thiazolidinediones
They are described separately because drugs in these
subclasses
Do not share a common mechanism of action
and
Are not structurally similar
29.
Biguanides
A biguanide refersto a structure where
Two guanidine molecules are linked through common
NH- link
Example: Phenformin, Metformin
Biguanides
Increase insulin sensitivity in liver and muscle
Inhibit glucose synthesis and release by the liver, and
Enhance the ability of tissues to take up glucose
It enhances insulin sensitivity and is not effective in the
absence of insulin
A biguanide differs from the sulfonylureas in
Not stimulating insulin secretion
Hence, generally does not cause hypoglycemia, even in large
doses
30.
Biguanides
Metformin
Currently theonly biguanide, acts by reducing hepatic glucose
production, largely by inhibiting gluconeogenesis and increasing
insulin sensitivity in muscle and fat cells
These actions are mediated at least partly by activation of
AMP-activated protein kinase (AMP kinase)
May be used alone or in combination with the sulfonylureas
A very important property is its ability to reduce hyperlipidemia
(LDL and VLDL cholesterol concentrations fall and HDL cholesterol
rises)
The patient often loses weight
Considered by some experts as the drug of choice in newly
diagnosed Type II diabetics
• Adverse effects are largely gastrointestinal, including diarrhea,
nausea, abdominal discomfort
• Lactic acidosis, a serious often fatal side effect associated with
biguanides, is rare in metformin
31.
Biguanides
Metformin
The liver normallyreleases glucose by detecting the level of
circulating insulin
When insulin levels are high, glucose is available in the blood,
and the liver produces little or no glucose
When insulin levels are low, there is little circulating glucose, so
the liver produces more glucose
In type 2 diabetes the liver may not detect levels of glucose in the
blood and, instead of regulating glucose production, releases
glucose despite blood sugar levels
Metformin sensitizes the liver
To circulating insulin levels and reduces hepatic glucose
production
The only drug that has been demonstrated to reduce
macrovascular events in type 2 DM
32.
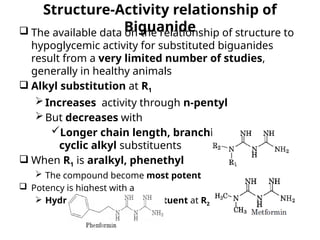
Structure-Activity relationship of
Biguanide
The available data on the relationship of structure to
hypoglycemic activity for substituted biguanides
result from a very limited number of studies,
generally in healthy animals
Alkyl substitution at R1
Increases activity through n-pentyl
But decreases with
Longer chain length, branching, or with
cyclic alkyl substituents
When R1 is aralkyl, phenethyl
The compound become most potent
Potency is highest with a
Hydrogen or methyl substituent at R2
33.
Thiazolidinediones
They are themost recently introduced class of oral
agents for treatment of type 2 diabetes
Improving insulin sensitivity and lowering blood
glucose, free fatty acid, and triglyceride levels
They are a group of structurally related peroxisome
proliferator-activated receptor γ (PPARγ) agonists
The PPARγ receptor is a member of the nuclear
hormone receptor family of ligand-activated
transcription factors that
Regulates gene expression of several genes
involved in fatty acid and carbohydrate
metabolism and adipocyte differentiation
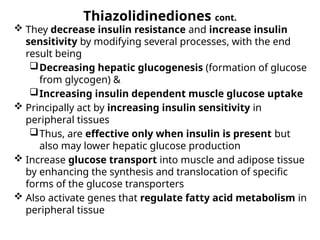
34.
Thiazolidinediones cont.
Theydecrease insulin resistance and increase insulin
sensitivity by modifying several processes, with the end
result being
Decreasing hepatic glucogenesis (formation of glucose
from glycogen) &
Increasing insulin dependent muscle glucose uptake
Principally act by increasing insulin sensitivity in
peripheral tissues
Thus, are effective only when insulin is present but
also may lower hepatic glucose production
Increase glucose transport into muscle and adipose tissue
by enhancing the synthesis and translocation of specific
forms of the glucose transporters
Also activate genes that regulate fatty acid metabolism in
peripheral tissue
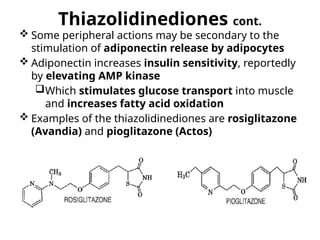
35.
Thiazolidinediones cont.
Someperipheral actions may be secondary to the
stimulation of adiponectin release by adipocytes
Adiponectin increases insulin sensitivity, reportedly
by elevating AMP kinase
Which stimulates glucose transport into muscle
and increases fatty acid oxidation
Examples of the thiazolidinediones are rosiglitazone
(Avandia) and pioglitazone (Actos)
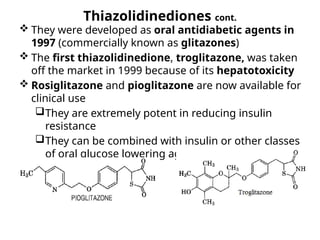
36.
Thiazolidinediones cont.
Theywere developed as oral antidiabetic agents in
1997 (commercially known as glitazones)
The first thiazolidinedione, troglitazone, was taken
off the market in 1999 because of its hepatotoxicity
Rosiglitazone and pioglitazone are now available for
clinical use
They are extremely potent in reducing insulin
resistance
They can be combined with insulin or other classes
of oral glucose lowering agents
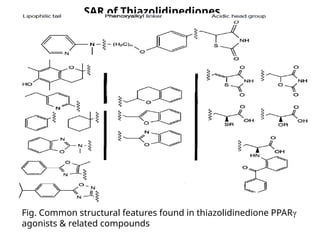
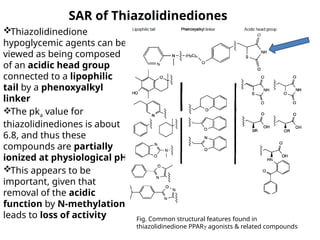
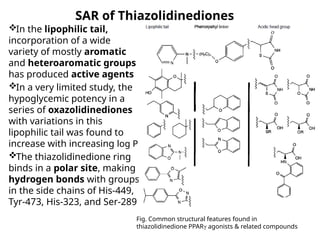
SAR of Thiazolidinediones
Thiazolidinedione
hypoglycemicagents can be
viewed as being composed
of an acidic head group
connected to a lipophilic
tail by a phenoxyalkyl
linker
The pka value for
thiazolidinediones is about
6.8, and thus these
compounds are partially
ionized at physiological pH
This appears to be
important, given that
removal of the acidic
function by N-methylation
leads to loss of activity Fig. Common structural features found in
thiazolidinedione PPARγ agonists & related compounds
39.
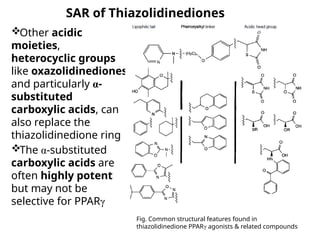
SAR of Thiazolidinediones
Otheracidic
moieties,
heterocyclic groups
like oxazolidinediones
and particularly α-
substituted
carboxylic acids, can
also replace the
thiazolidinedione ring
The α-substituted
carboxylic acids are
often highly potent
but may not be
selective for PPARγ
Fig. Common structural features found in
thiazolidinedione PPARγ agonists & related compounds
40.
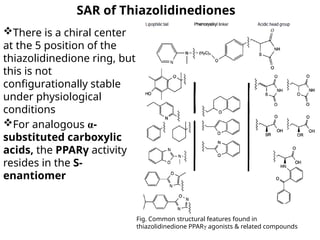
SAR of Thiazolidinediones
Thereis a chiral center
at the 5 position of the
thiazolidinedione ring, but
this is not
configurationally stable
under physiological
conditions
For analogous α-
substituted carboxylic
acids, the PPARγ activity
resides in the S-
enantiomer
Fig. Common structural features found in
thiazolidinedione PPARγ agonists & related compounds
41.
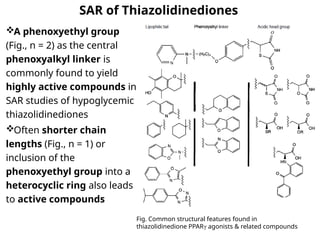
SAR of Thiazolidinediones
Aphenoxyethyl group
(Fig., n = 2) as the central
phenoxyalkyl linker is
commonly found to yield
highly active compounds in
SAR studies of hypoglycemic
thiazolidinediones
Often shorter chain
lengths (Fig., n = 1) or
inclusion of the
phenoxyethyl group into a
heterocyclic ring also leads
to active compounds
Fig. Common structural features found in
thiazolidinedione PPARγ agonists & related compounds
42.
SAR of Thiazolidinediones
Inthe lipophilic tail,
incorporation of a wide
variety of mostly aromatic
and heteroaromatic groups
has produced active agents
In a very limited study, the
hypoglycemic potency in a
series of oxazolidinediones
with variations in this
lipophilic tail was found to
increase with increasing log P
The thiazolidinedione ring
binds in a polar site, making
hydrogen bonds with groups
in the side chains of His-449,
Tyr-473, His-323, and Ser-289
Fig. Common structural features found in
thiazolidinedione PPARγ agonists & related compounds
43.
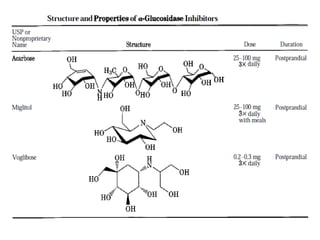
α-Glucosidase Inhibitors
Lowerblood glucose by delaying the
Digestion of carbohydrates and
Absorption of carbohydrates in the intestine
E.g., Acarbose( Precose) and Miglitol (Glyset)
Reduce intestinal absorption of starch, dextrin, and
disaccharides by inhibiting the action of α-glucosidase in the
intestinal brush border
Consequent to this delayed carbohydrate absorption, the
postprandial rise in plasma glucose is blunted in both normal and
diabetic subjects
May be used
As monotherapy in elderly patients or
In patients with predominantly postprandial hyperglycemia
Typically are used in combination with other oral antidiabetic
agents and/or insulin
The drugs should be administered at the start of a meal
44.
α-Glucosidase Inhibitors cont.
Acarbose
Inhibits α-glucosidase in the intestinal brush border
Thus, decreases the absorption of starch and disaccharides
Consequently the postprandial rise of blood glucose is blunted
Unlike the other oral hypoglycemic agents, acarbose does
not
Stimulate insulin release from the pancreas nor does it
increase insulin action in peripheral tissues
Thus, does not cause hypoglycemia
Can be used
As monotherapy in those patients being controlled by
diet or
In combination with other oral hypoglycemic agents,
or with insulin
It is poorly absorbed and its major side effects are
flatulence, diarrhea, and abdominal cramping
#21 An ATP-sensitive potassium channel (or KATP channel) is a type of potassium channel that is gated by intracellular nucleotides,ATP and ADP. ATP-sensitive potassium channels are composed of Kir6.x-type subunits and sulfonylurea receptor (SUR) subunits, along with additional components


































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)







![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)