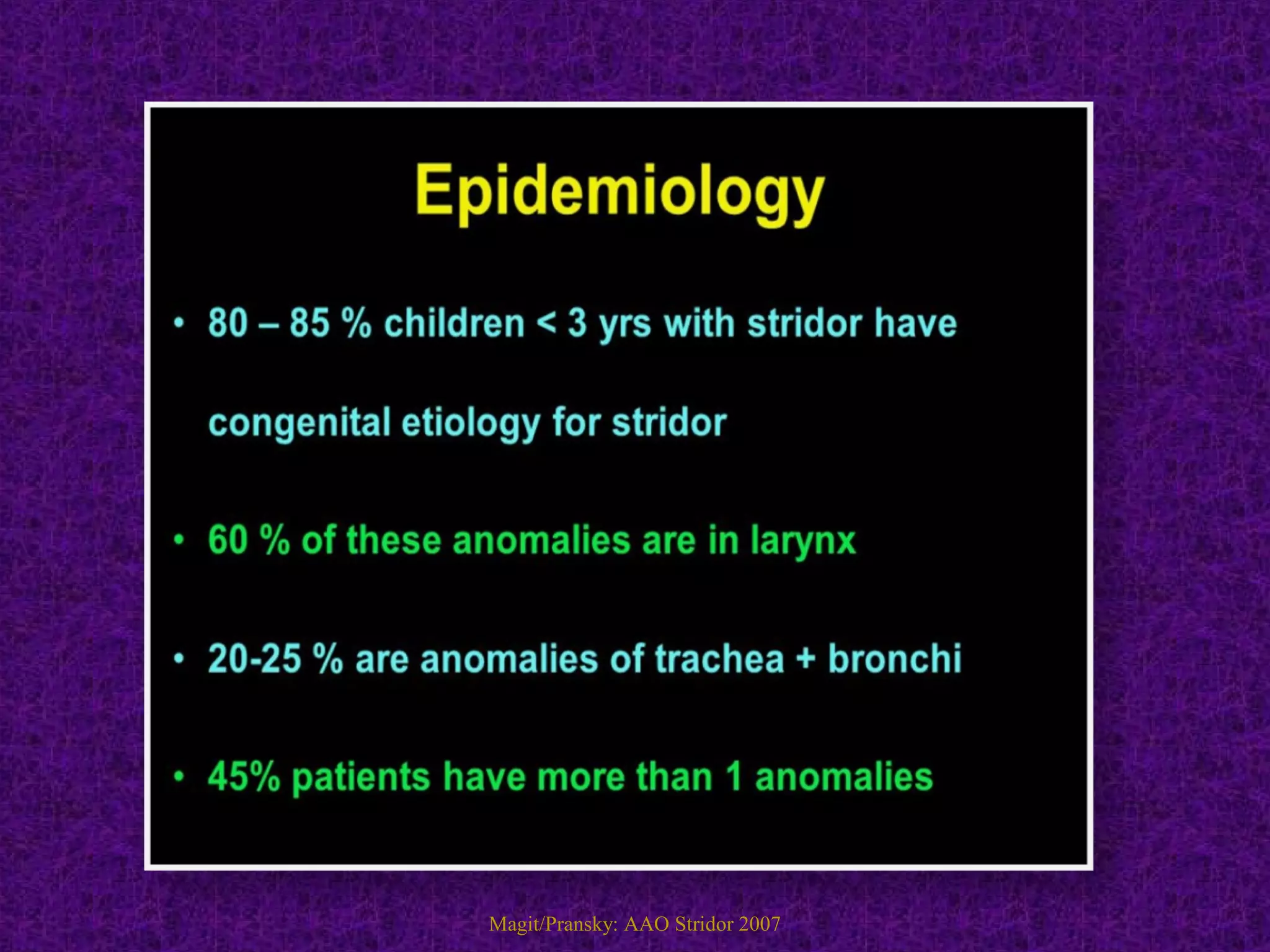
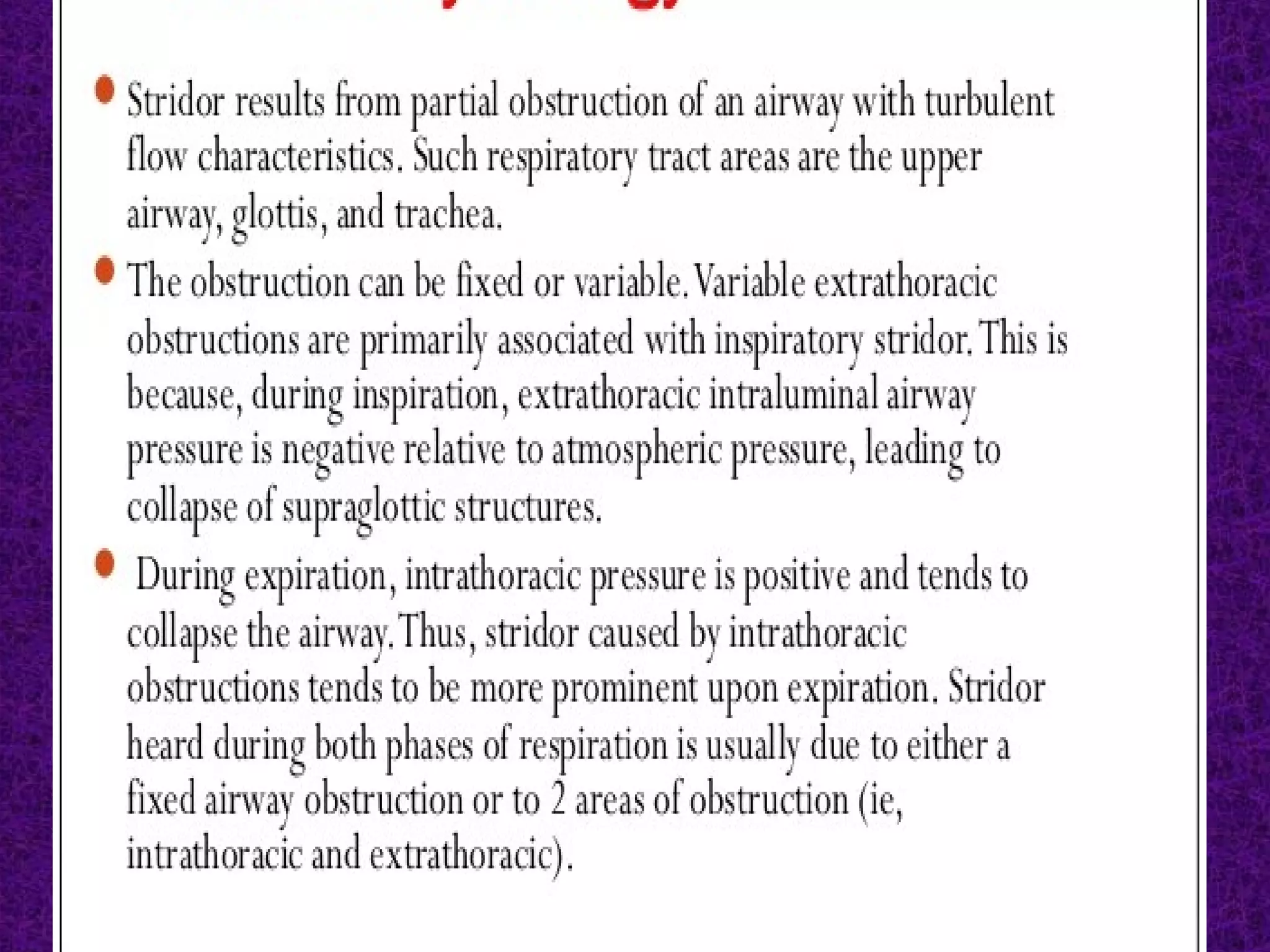
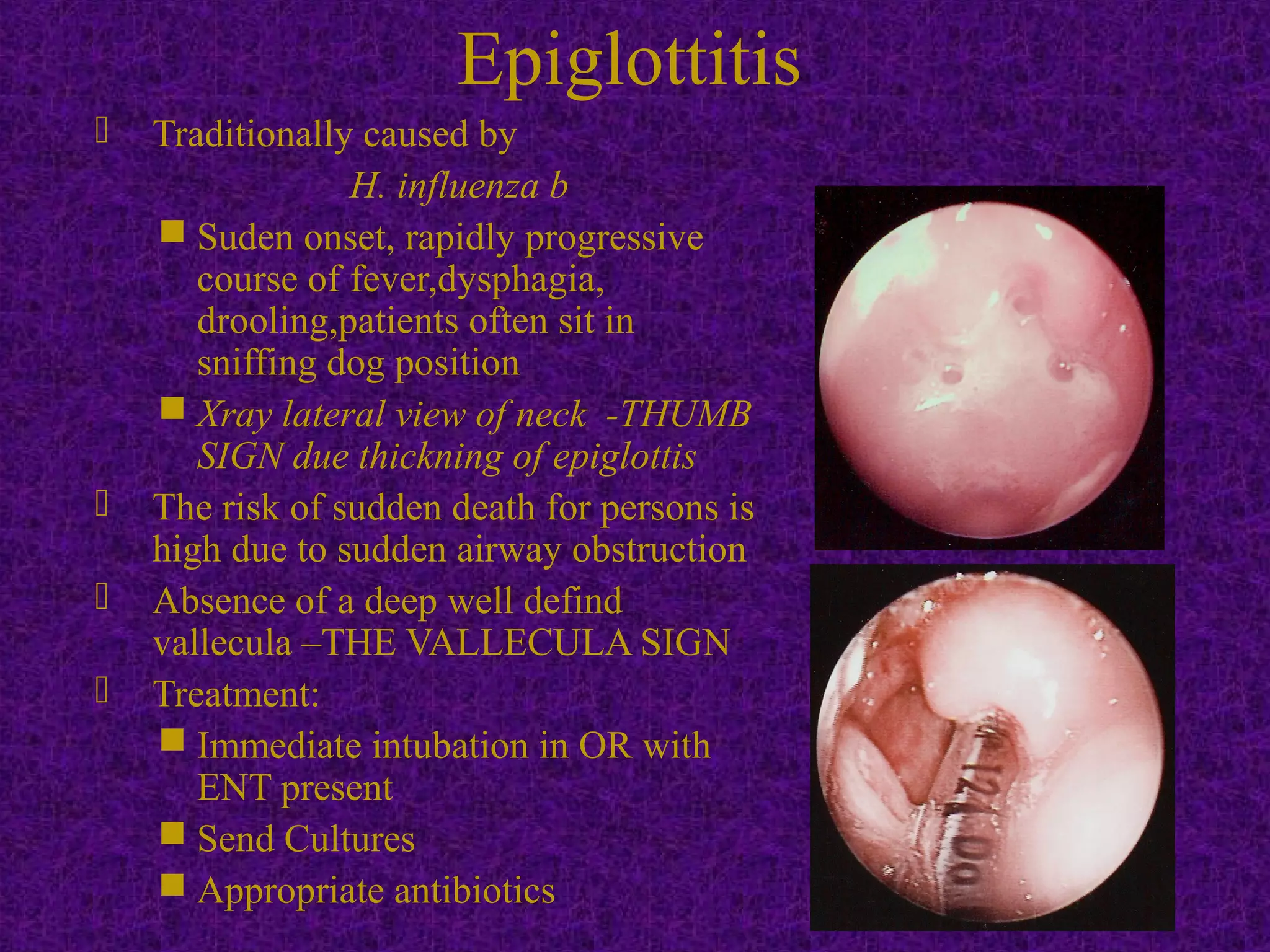
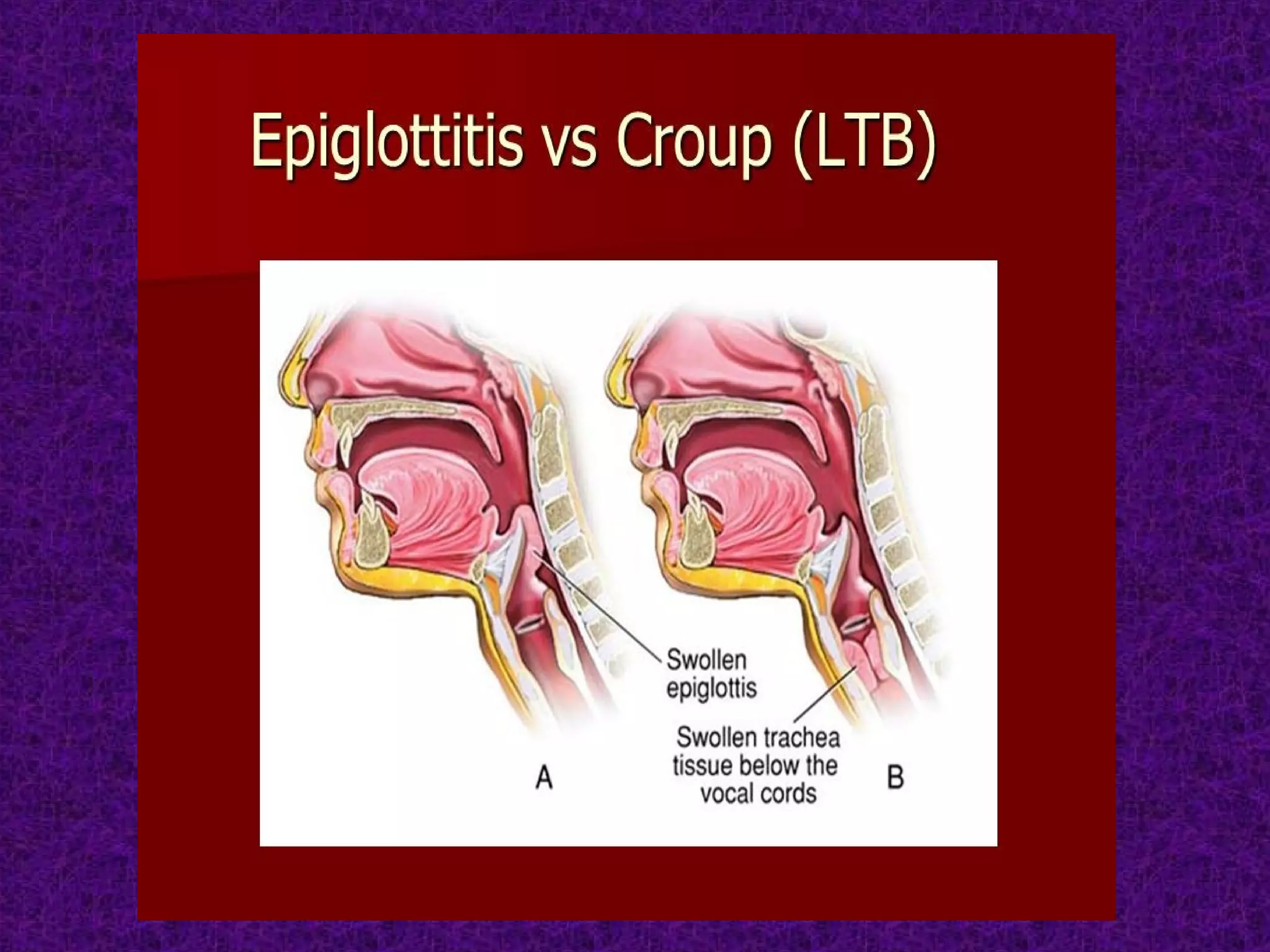
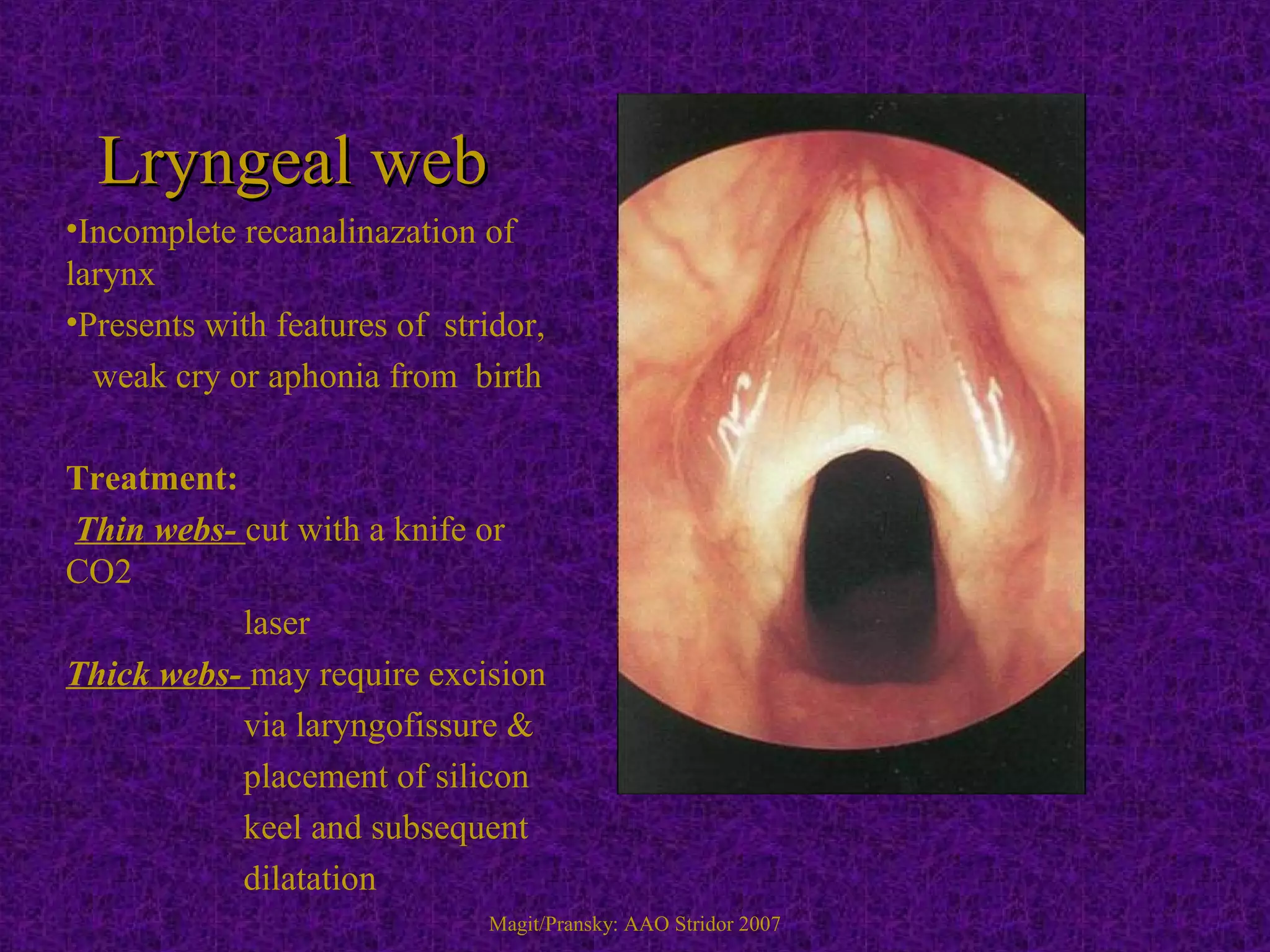
Stridor is an abnormal high-pitched noise caused by partial airway obstruction. In children, chronic stridor is usually due to congenital lesions like laryngomalacia, while acute stridor is often caused by infections. In adults, chronic stridor indicates a serious underlying pathology such as laryngeal carcinoma. Common causes of stridor include laryngomalacia, vocal cord paralysis, infections like croup, epiglottitis, and foreign body aspiration. Evaluation involves history, examination, imaging like X-rays and laryngoscopy. Treatment depends on the cause but may include oxygen, steroids, intubation, tracheostomy, or surgery.