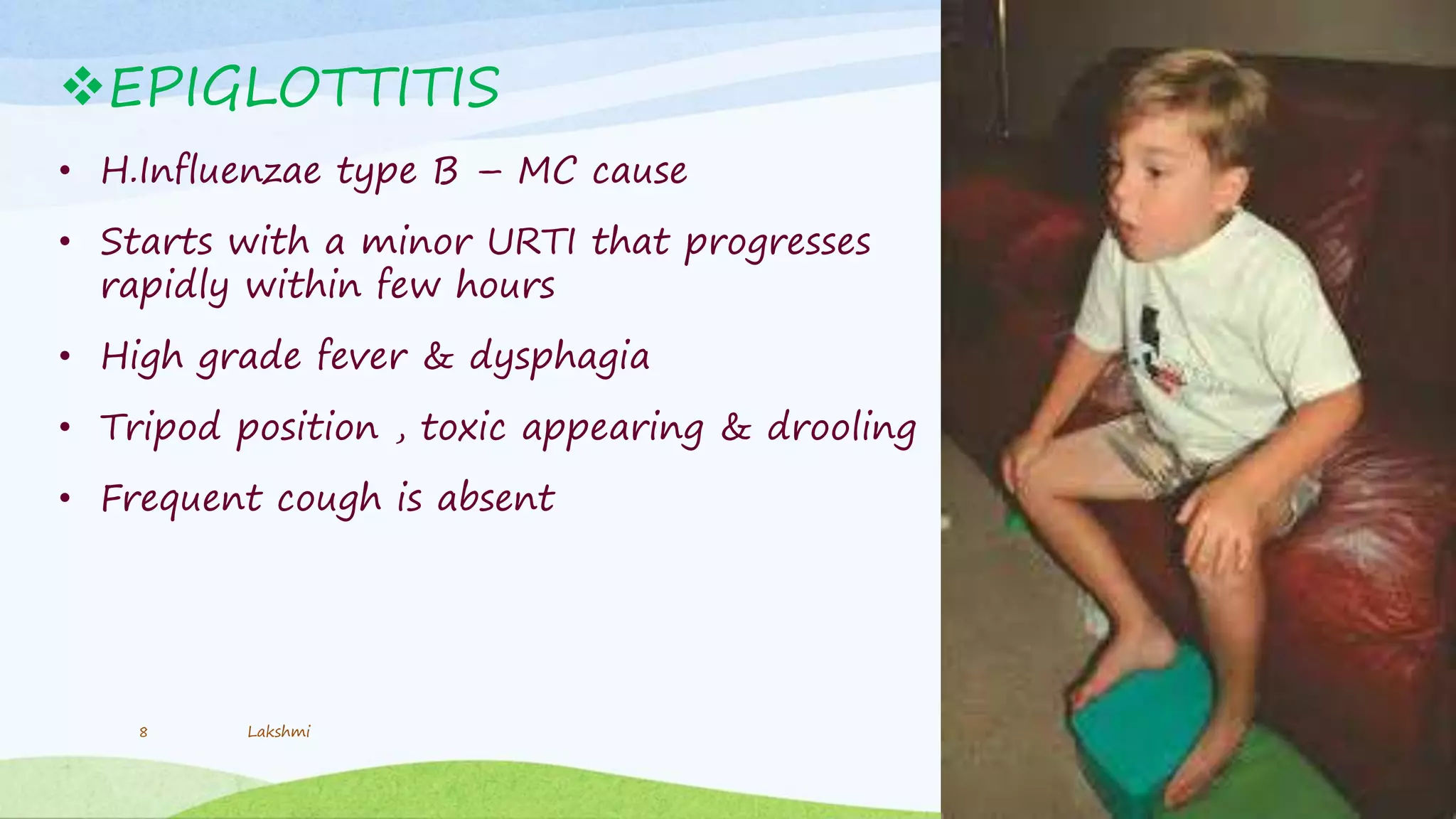
Stridor is a noisy, high-pitched breathing sound caused by upper airway obstruction. It is common in infants due to their small larynx size and loose tissues. The relationship of stridor to inspiration and expiration can provide clues to its cause. Acute stridor is usually due to inflammation and edema causing supraglottic or subglottic obstruction. Common causes include croup, epiglottitis, and infections. Chronic stridor may be due to congenital abnormalities, neurogenic issues, or tumors. Evaluation involves history, examination, and endoscopy. Management depends on the specific cause but may include antibiotics, steroids, intubation, or surgery.