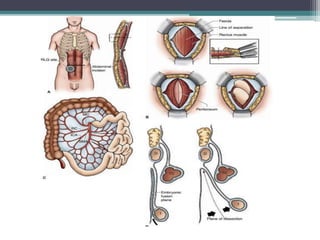
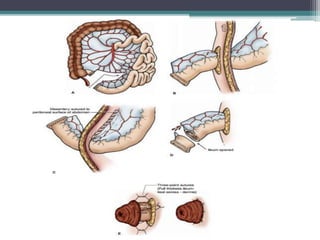
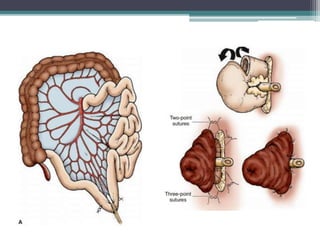
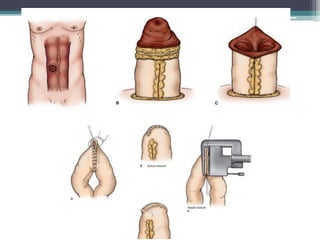
This document discusses different types of intestinal stomas. It begins by defining a stoma as an opening of the intestinal tract onto the abdominal wall, which can be temporary or permanent. It describes factors to consider when selecting a stoma site, such as avoiding deep folds of fat or scars. The document then covers various types of stomas including colostomies and ileostomies. It provides details on their construction, functions, and post-operative care considerations. In summary, the document provides an overview of intestinal stomas, how they are formed and classified, as well as best practices for patient aftercare.





![Basics of Stoma and Management care[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/basicsofstomaandmanagement1-250417022629-8799f789-thumbnail.jpg?width=640&height=640&fit=bounds)









































![[DSC Europe 25] Josip Saban - Career building for data professionals.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/zroflcttkm1vmli0txea-josip-saban-career-building-for-data-professionals-260123083019-587cdb8c-thumbnail.jpg?width=640&height=640&fit=bounds)
