Downloaded 13 times
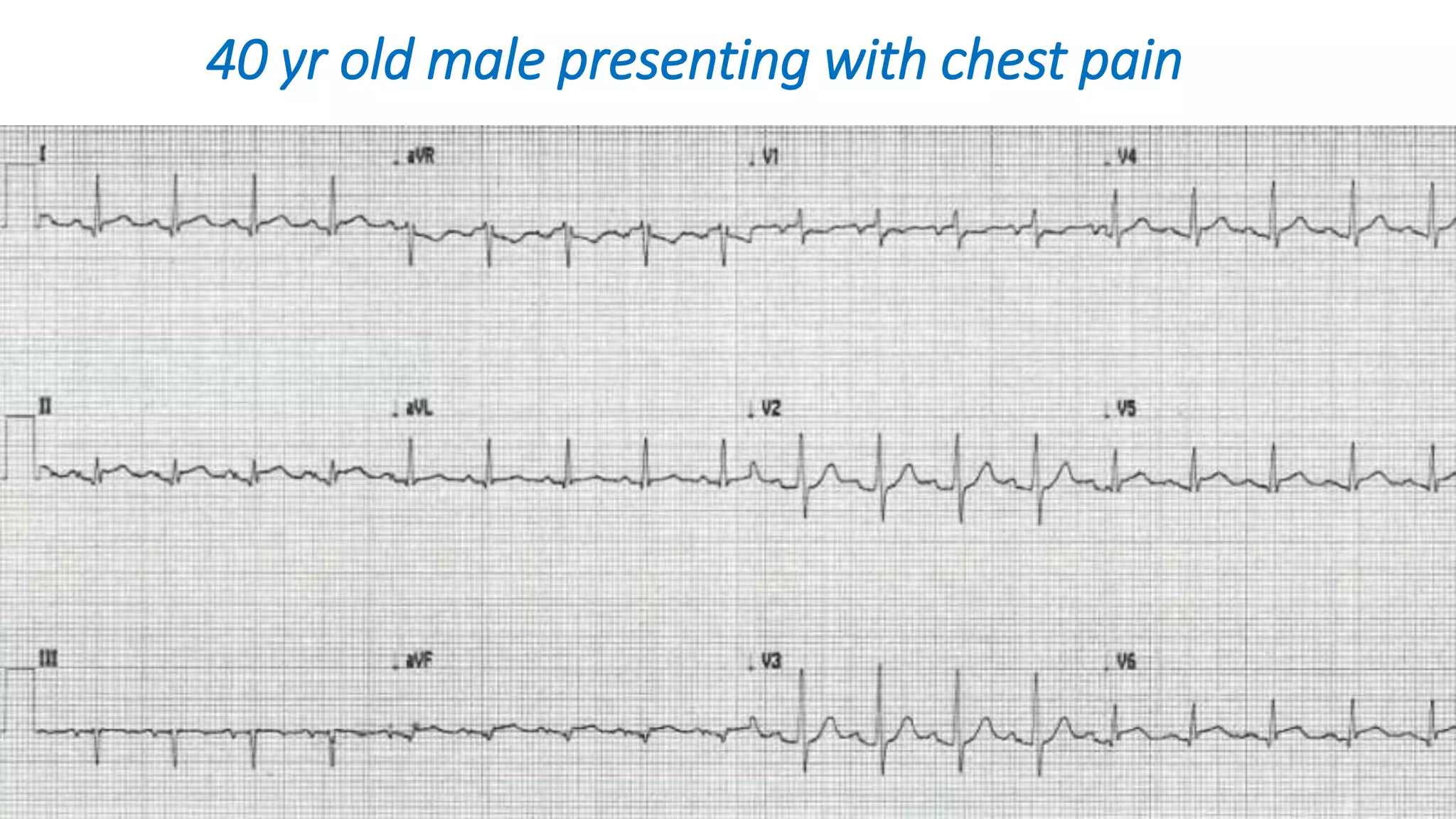


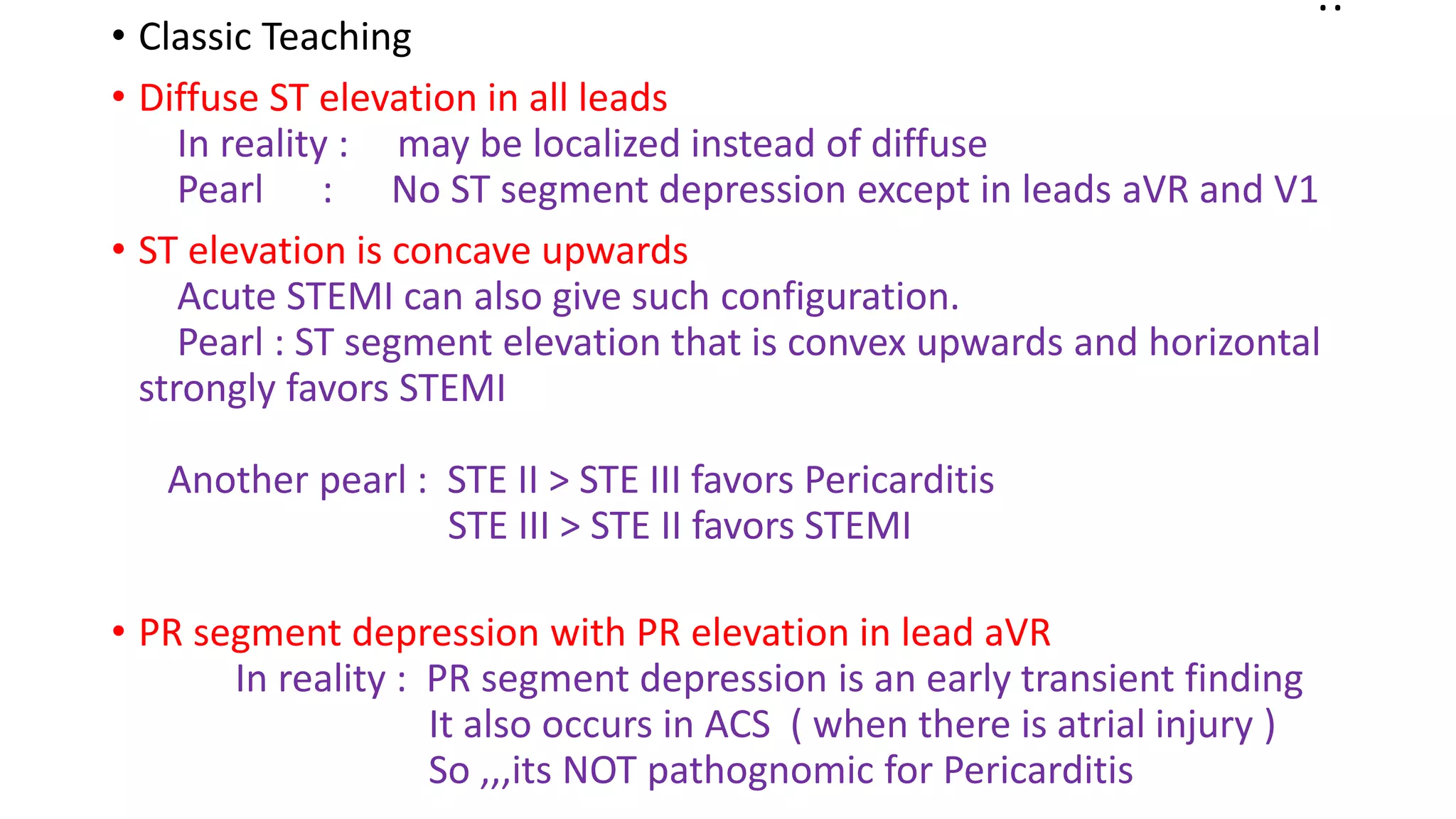
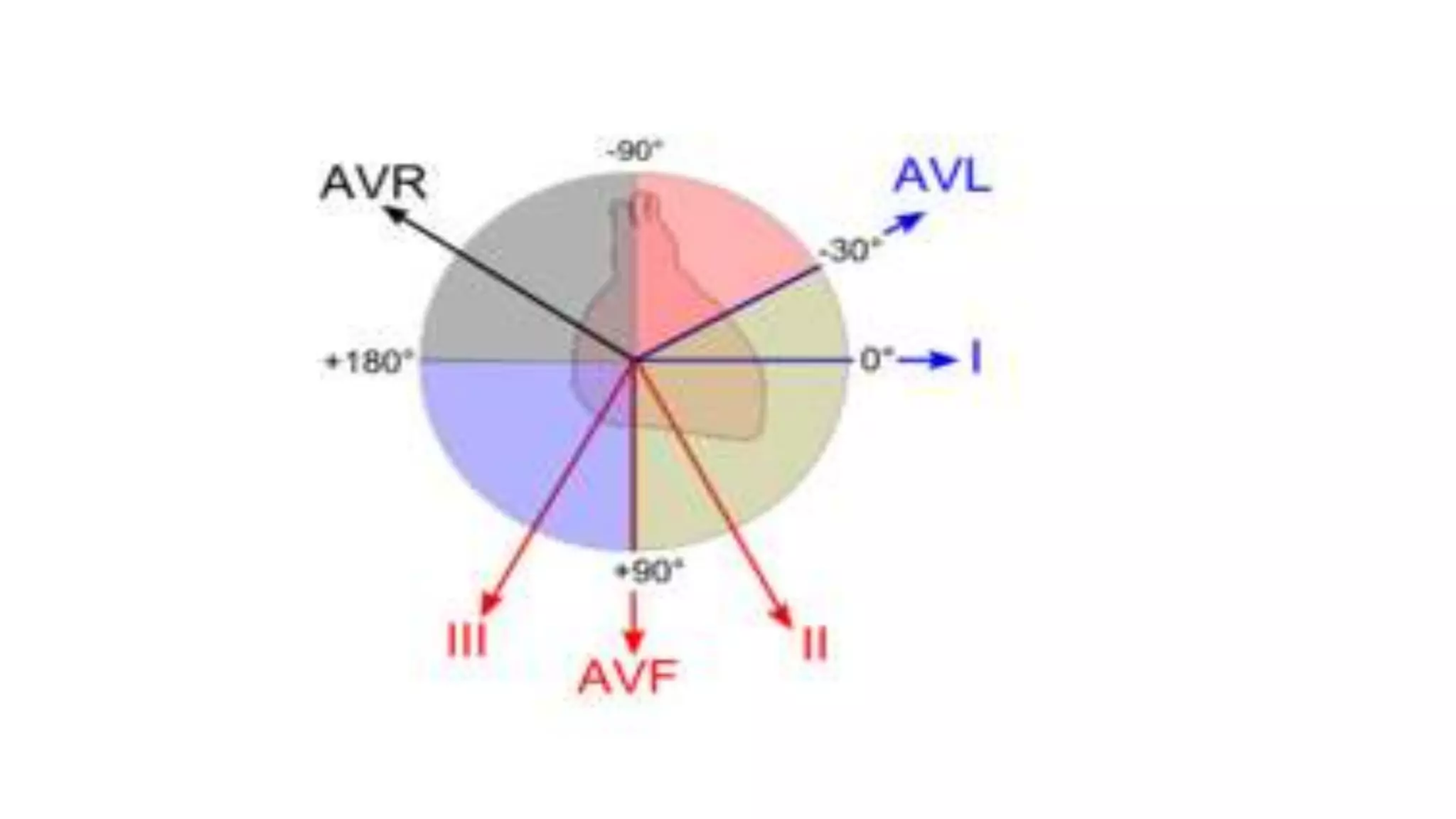

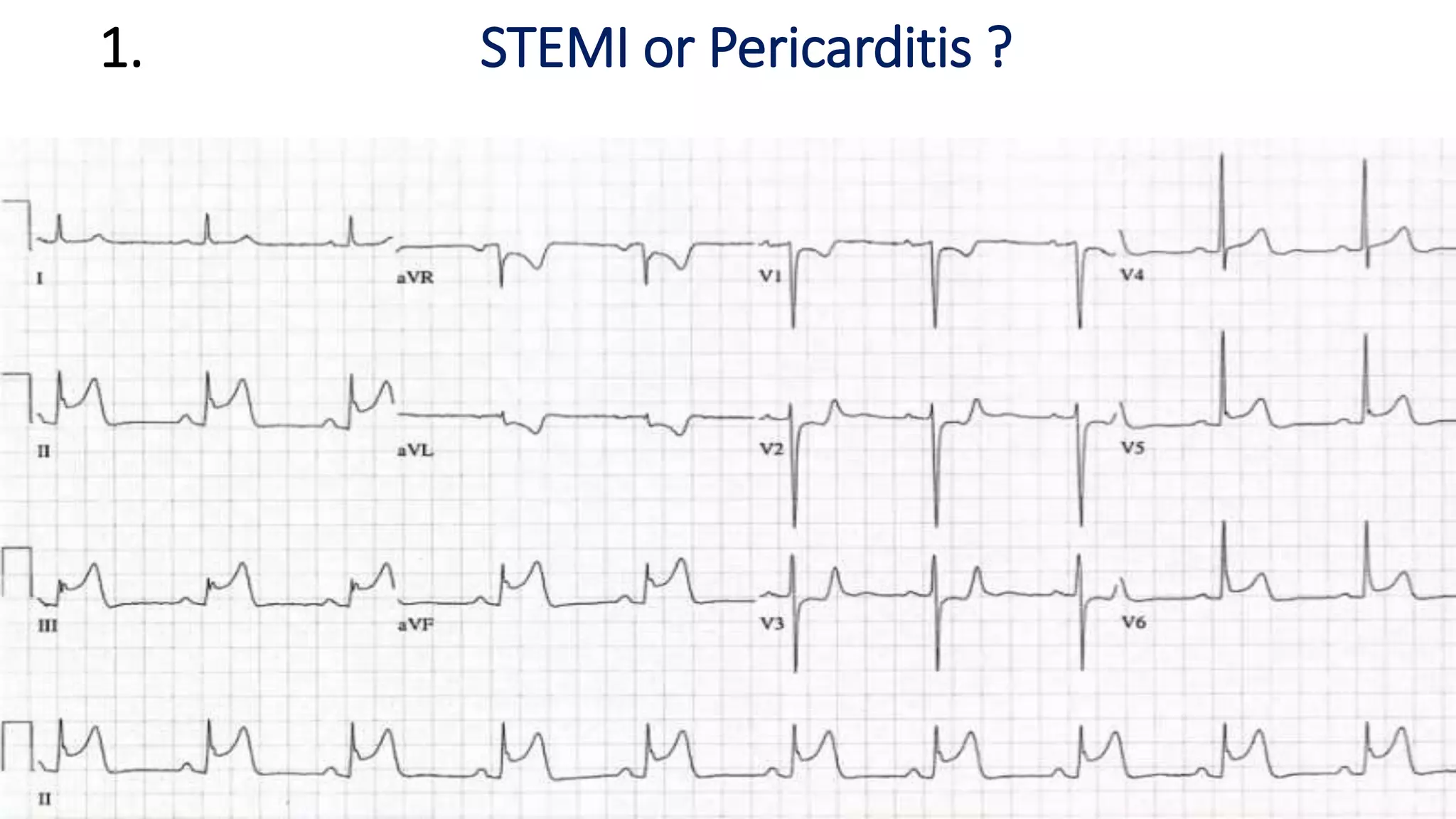

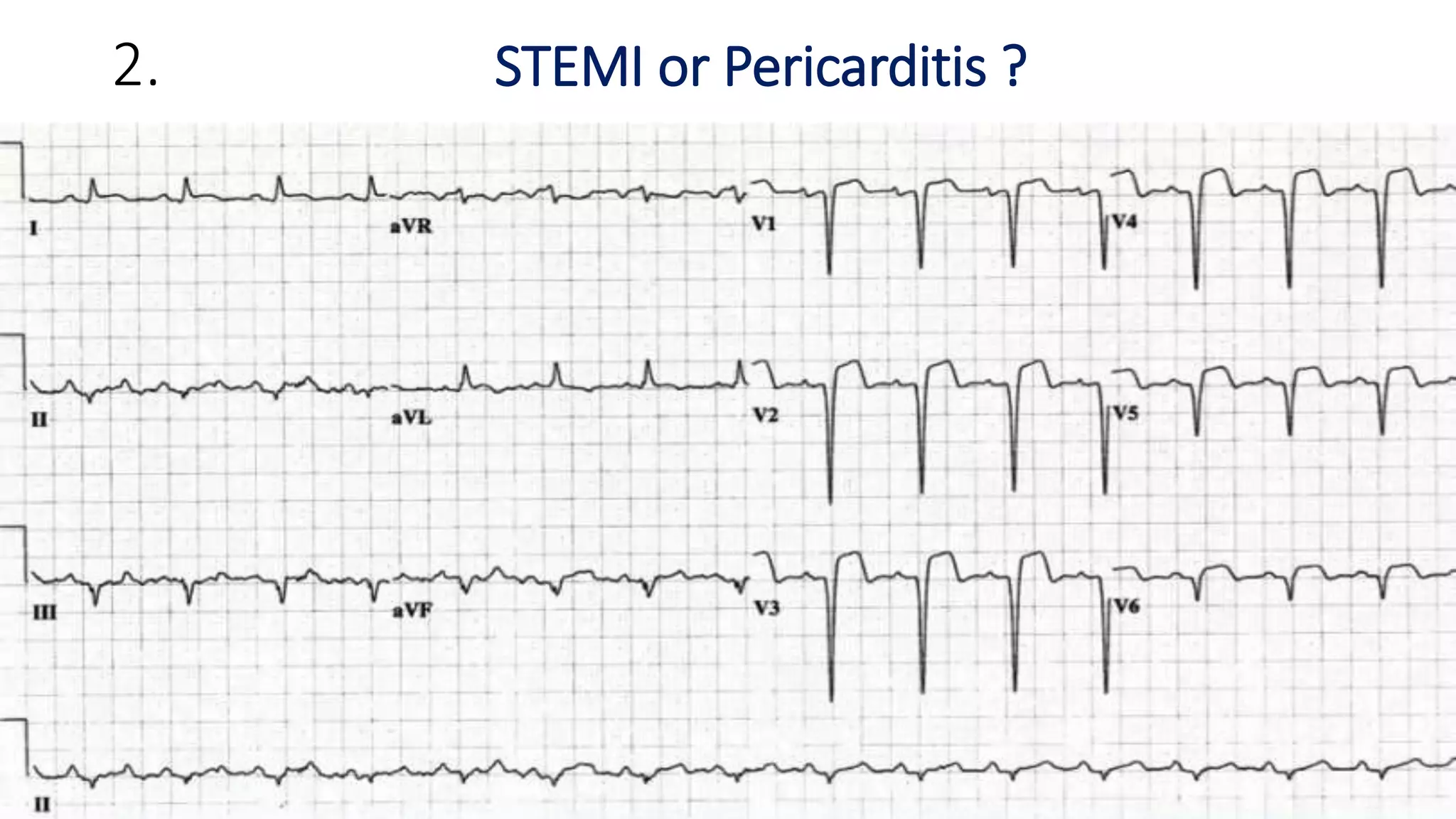

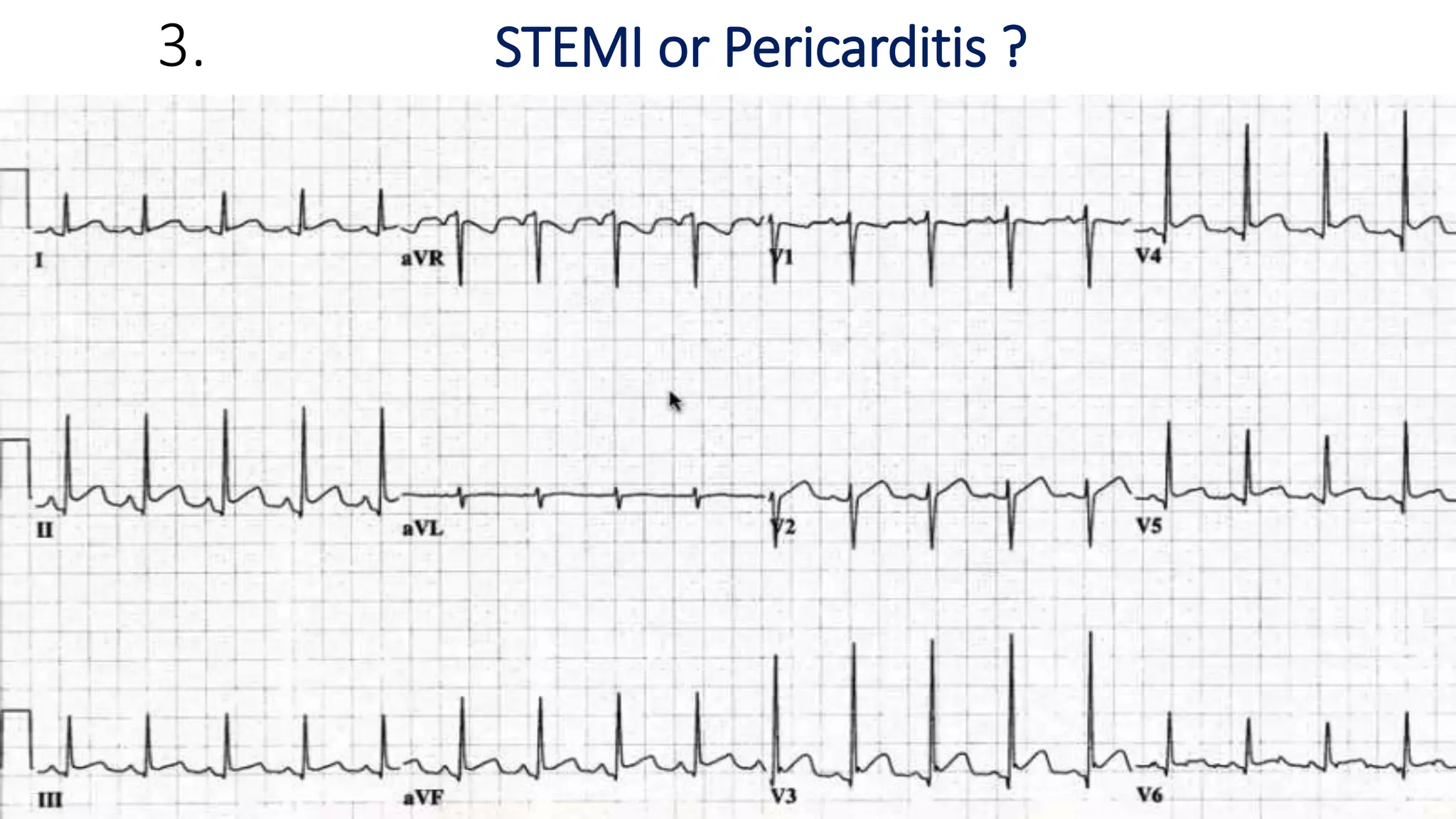


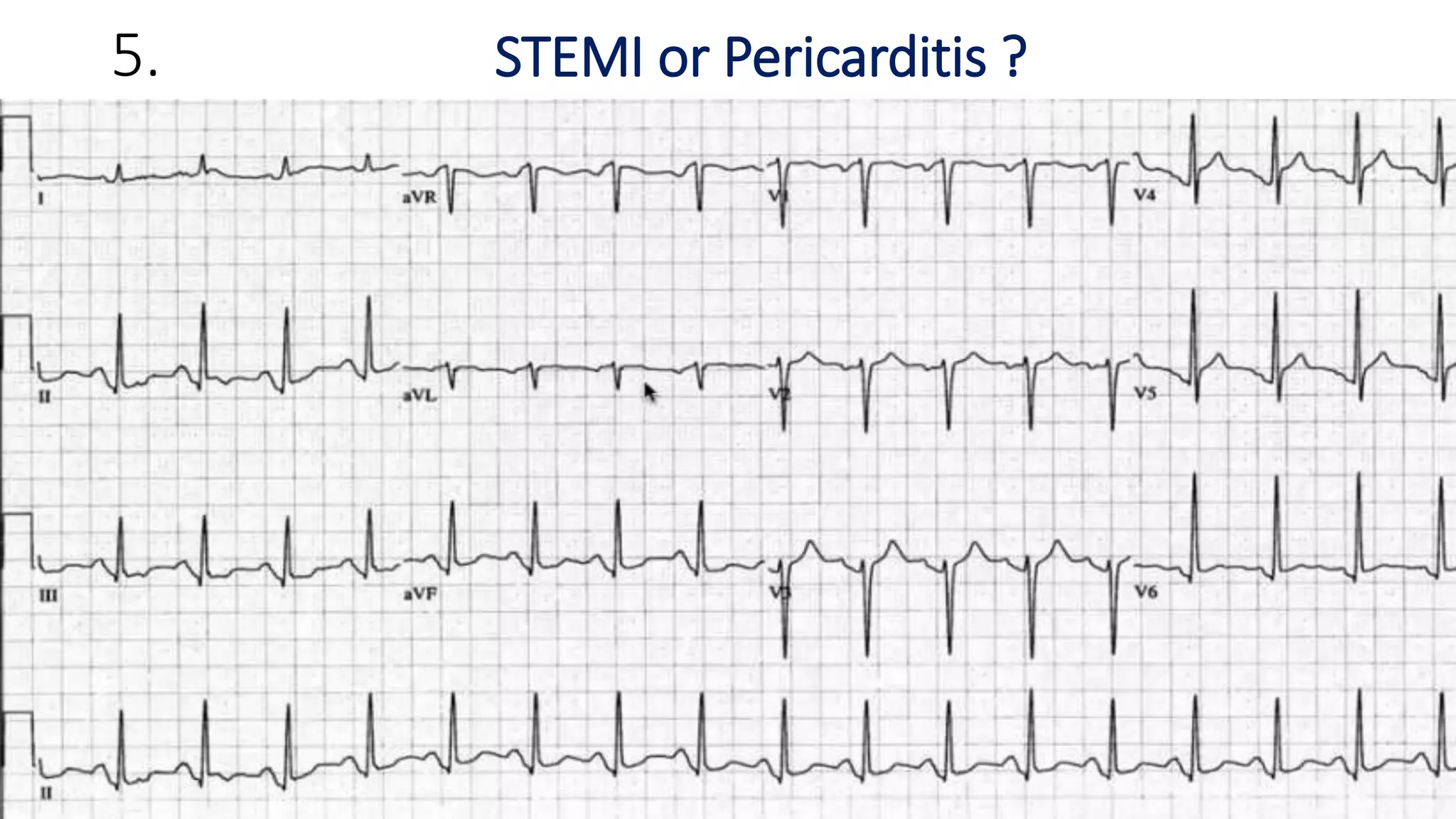






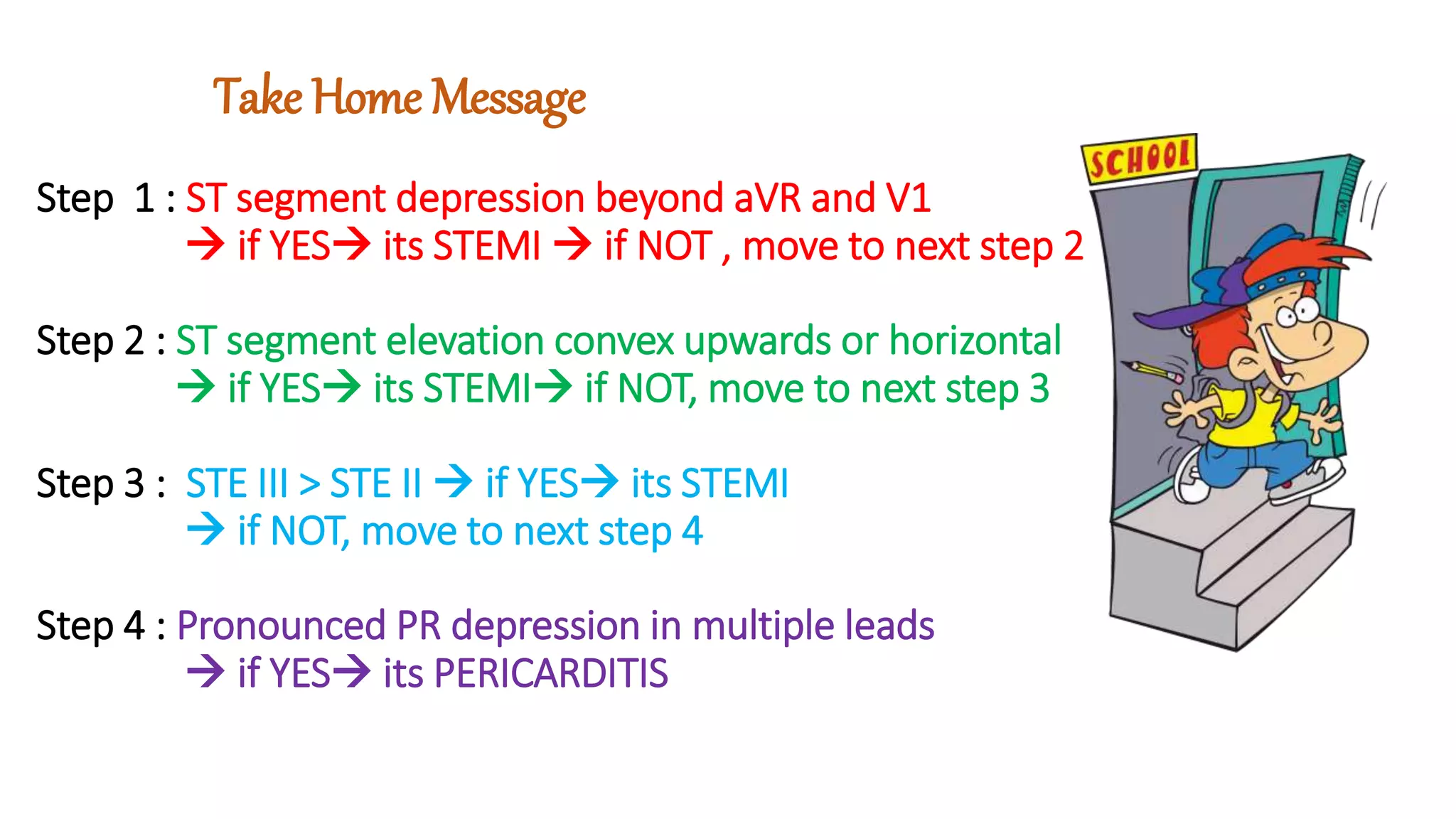


This document discusses the challenges in differentiating between ST elevation myocardial infarction (STEMI) and pericarditis based on electrocardiogram (ECG) findings. While pericarditis is classically taught to present with diffuse ST elevation and PR segment depression, in reality the findings can be more localized. STEMI can also occasionally present with concave ST elevation. The document provides factors that favor STEMI over pericarditis, including ST depression beyond leads aVR and V1, convex or horizontal ST elevation, and greater ST elevation in lead III than II. It emphasizes getting serial ECGs when the diagnosis is unclear and discusses an example where PR depression occurred due to atrial injury in the setting of acute










































































