
Download to read offline



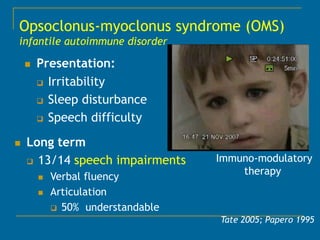








This document discusses the cognitive and psychiatric phenotypes associated with several pediatric movement disorders. It provides examples of children who presented with psychiatric symptoms like irritability, temper tantrums, and psychosis but were ultimately diagnosed with physical conditions causing their movements disorders like hemichorea, opsoclonus-myoclonus syndrome, Tourette syndrome, Wilson's disease, and restless leg syndrome. Many movement disorders are associated with long-term cognitive and psychiatric comorbidities like low IQ, behavioral issues, anxiety, and depression. Proper diagnosis and treatment of the underlying physical condition can help address both motor symptoms and comorbid mental health issues.

















![Etiopathogenesis of obsessive compulsive disorder [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/etiopathogenesisofobsessivecompulsivedisorderautosaved-170329074058-thumbnail.jpg?width=640&height=640&fit=bounds)
























































