Downloaded 677 times
![ETIOLOGY
Biological Factors
Serotonergic System
Clinical studies have assayed CSF concentrations of serotonin metabolites
(e.g., 5-hydroxyindoleacetic acid [5-HIAA]) and affinities and numbers of
platelet-binding sites of tritiated imipramine , which binds to serotonin
reuptake sites, and have reported variable findings of these measures in
patients with OCD. In one study, the CSF concentration of 5-HIAA decreased
after treatment with clomipramine , focusing attention on the serotonergic
system.](https://image.slidesharecdn.com/obsessive-compulsivedisorder-150617183013-lva1-app6892/85/Obsessive-compulsive-disorder-13-320.jpg)
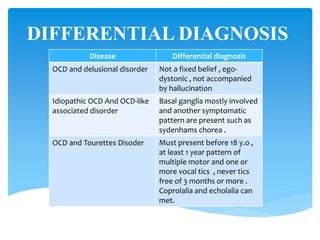
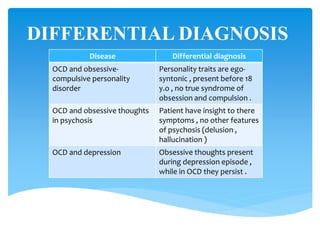

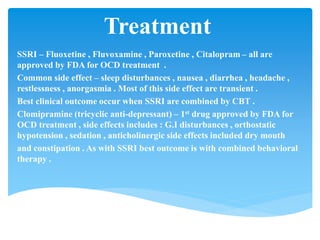
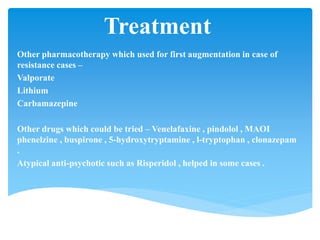



Obsessive-Compulsive Disorder (OCD) is an anxiety disorder characterized by intrusive thoughts and compulsive behaviors that cause significant distress and impact daily functioning. The condition affects an estimated 2-3% of the population and often co-occurs with other mental health disorders, such as major depression and anxiety. Treatment typically involves a combination of pharmacotherapy, primarily SSRIs, and cognitive-behavioral therapy, with more severe cases sometimes resolved through surgical options.



















































![Etiopathogenesis of obsessive compulsive disorder [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/etiopathogenesisofobsessivecompulsivedisorderautosaved-170329074058-thumbnail.jpg?width=640&height=640&fit=bounds)















































