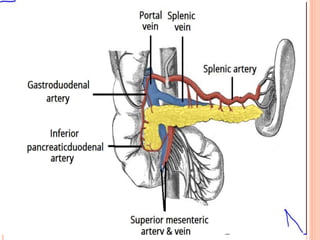
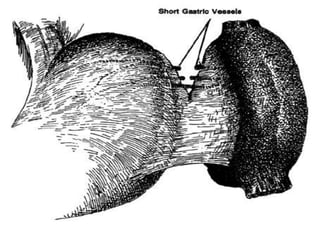
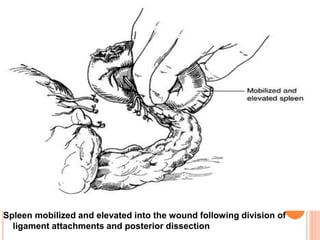
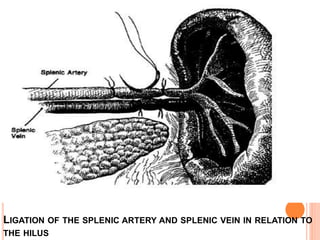
This document provides information on hypersplenism and its surgical management. It begins with definitions of hypersplenism and classifications of primary and secondary hypersplenism. The indications for splenectomy include bleeding varices, hereditary spherocytosis, massive splenic trauma, and others. The surgical technique involves mobilizing the spleen through ligation of attachments and dissection of the hilum before removing the spleen and ligating vessels. Precise ligation of the splenic artery and vein is important to safely remove an enlarged spleen.






































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)









