Downloaded 362 times
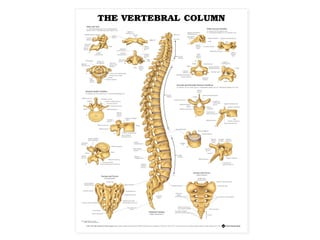
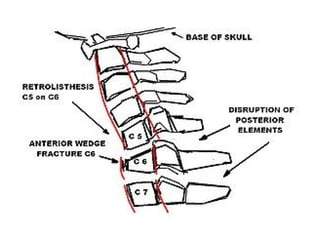





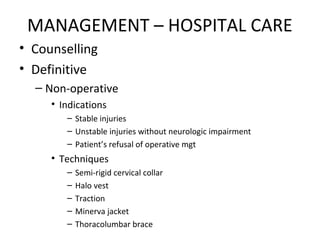

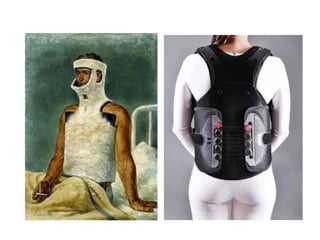
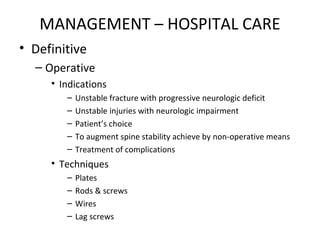
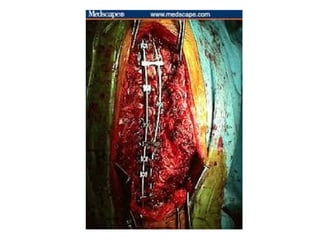


This document discusses spine injuries, including their definition, epidemiology, anatomy, classification, pathophysiology, diagnosis, management, rehabilitation, complications, prevention, and current trends. Spine injuries refer to damage to the bony or ligamentous structures of the spine, which can occur with or without neurological impairment. They are frequently caused by motor vehicle accidents or falls and require early recognition and treatment to achieve good outcomes. Management involves pre-hospital stabilization and transport, hospital evaluation and stabilization, and may include surgical or non-surgical techniques depending on the injury. Rehabilitation aims to prevent complications and promote recovery, while efforts should also focus on prevention to reduce the incidence of these often devastating injuries.





















































![Spinal cord injury [recovered]](https://cdn.slidesharecdn.com/ss_thumbnails/spinalcordinjuryrecovered-201022180848-thumbnail.jpg?width=640&height=640&fit=bounds)







![9 Spinal Cord Injury Sci [2]](https://cdn.slidesharecdn.com/ss_thumbnails/9spinalcordinjurysci2-100330221058-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)









































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

