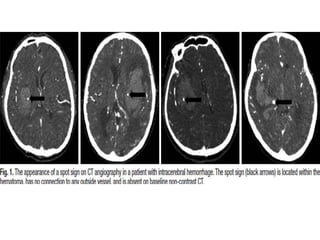
1. The document discusses a study comparing surgical treatment versus conservative treatment for patients with spontaneous intracerebral hemorrhage who are positive for the "spot sign" on imaging.
2. The study found that while mortality at 90 days was significantly lower in patients who received surgery, there was no significant difference in clinical outcomes like the Glasgow Outcome Scale between the surgical and conservative treatment groups.
3. Therefore, the study concludes that while surgery may reduce mortality risk, it does not clearly provide a clinical outcome benefit over conservative treatment for spot sign positive intracerebral hemorrhage patients.
![Exclusion criteria
1) Patients with poor or good neurologic status [Glasgow Coma Scale (GCS) 3–5, or
15]
2) Brain stem hemorrhage and cerebellar hemorrhage.
3) A previous stroke history with neurological deficits.
4) Pure intraventricular hemorrhage (IVH)
5) Secondary intracerebral hemorrhage such as arteriovenous malformation,
moyamoya disease, tumor bleeding, and venous sinus thrombosis.
6) Incompletion of a standard CT protocol including noncontrast CT (NCCT) and
MDCTA.
7) Cortical hemorrhage
8) Refuse surgical treatment despite of surgical indication.](https://image.slidesharecdn.com/journalclubnew-170920123341/85/Journal-club-new-6-320.jpg)