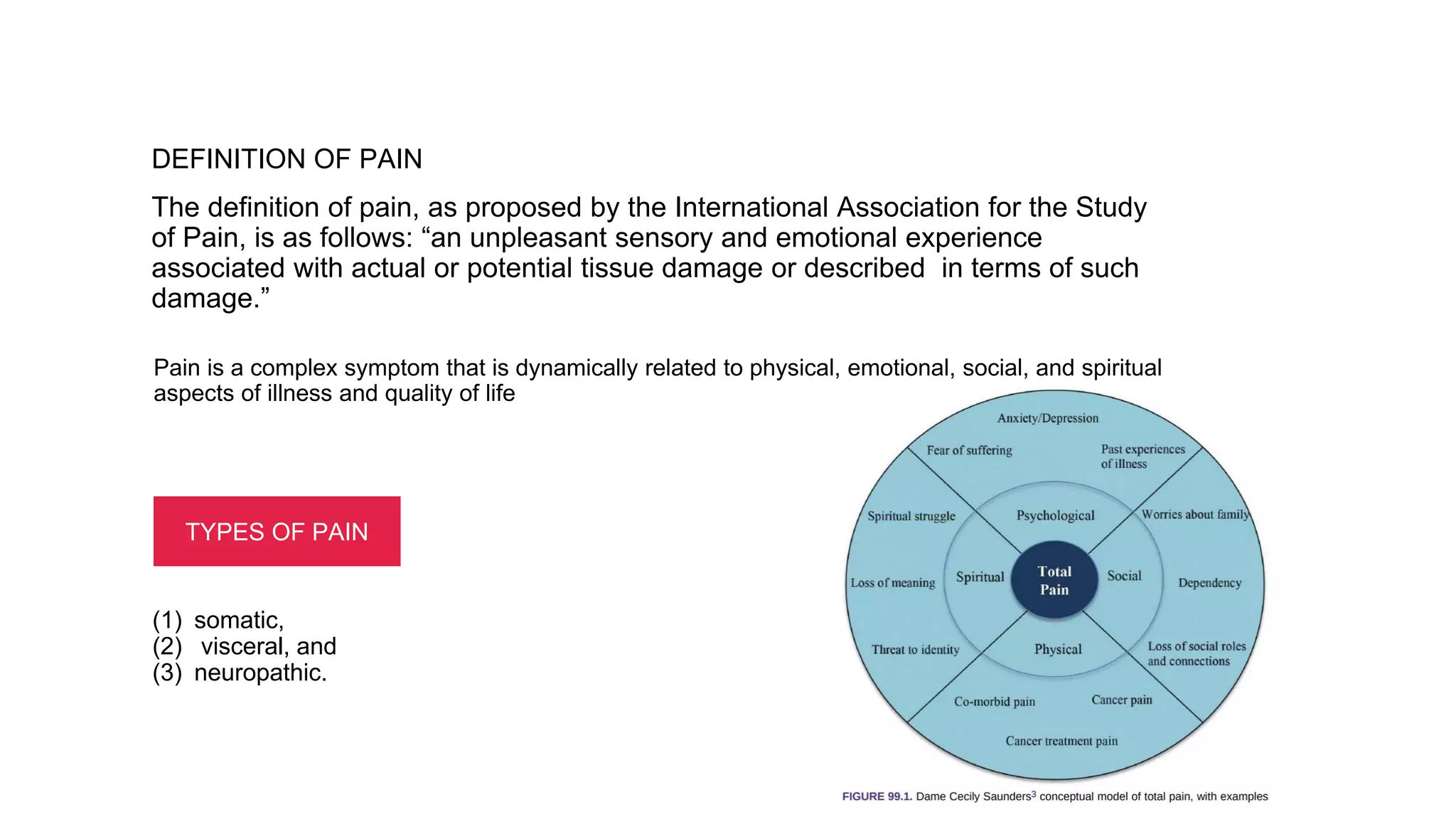
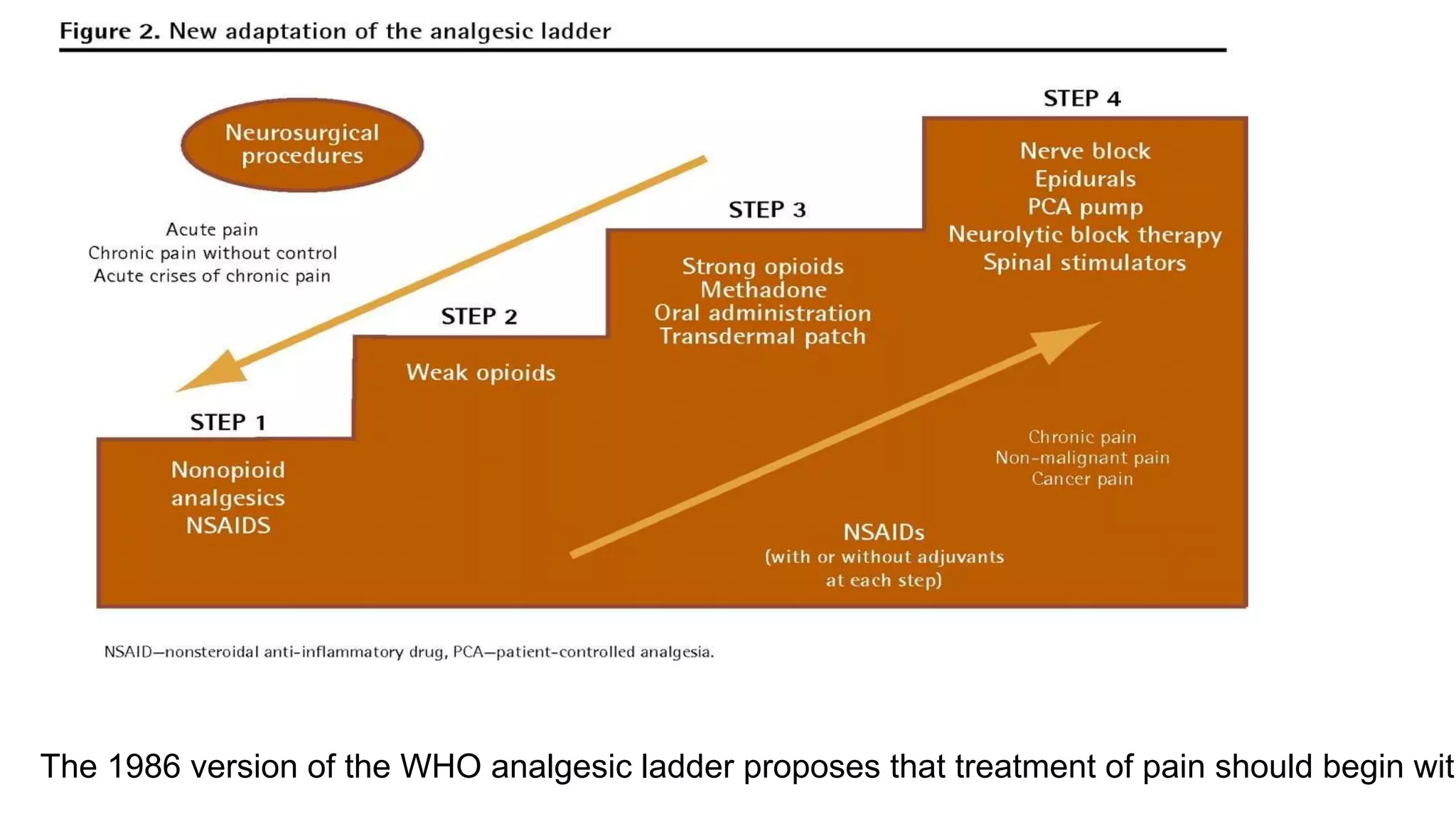
This document discusses pain management in cancer patients. It defines pain and describes the different types of pain. It discusses the pathophysiology of pain pathways and various scales used to assess and grade a patient's pain. It also discusses barriers to effective pain management and the WHO analgesic ladder for treating cancer pain with non-opioid and opioid medications like paracetamol, NSAIDs, tramadol, morphine, fentanyl, and methadone. Adjuvant therapies and alternative treatments are also mentioned.