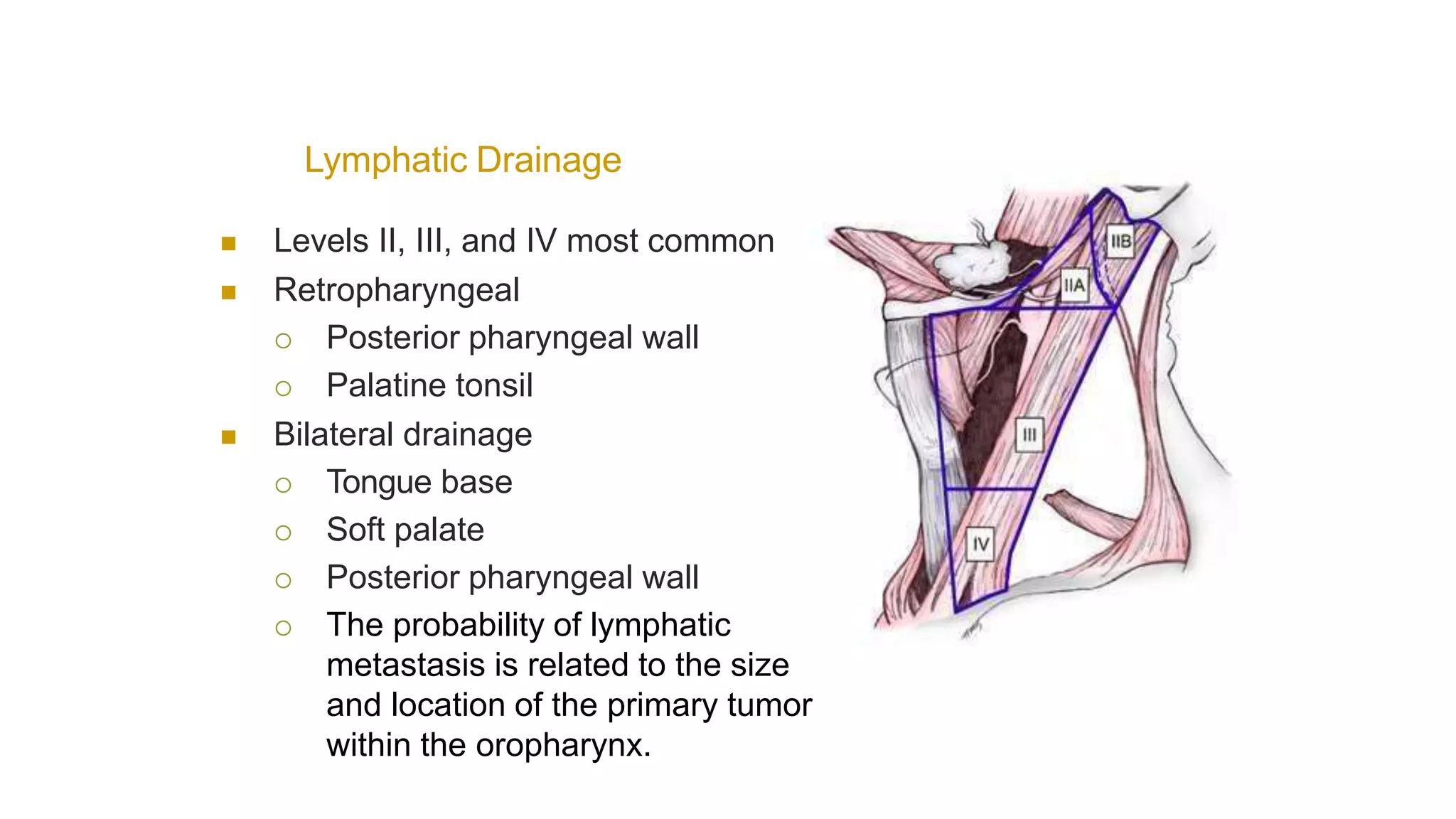
The document discusses management of oropharyngeal cancers. The oropharynx includes areas like the base of the tongue, soft palate, tonsils and posterior pharyngeal walls. Oropharyngeal cancers commonly spread to cervical lymph nodes in levels II, III and IV. Risk factors include age, gender, smoking, alcohol and HPV infection. Treatment may involve surgery, radiation therapy or chemotherapy depending on the stage of cancer. Imaging tests like CT, MRI and PET scans are used to stage the cancer and detect metastases.