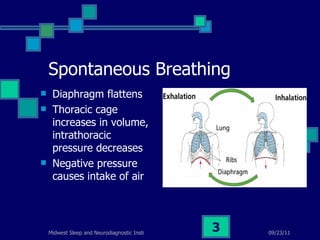
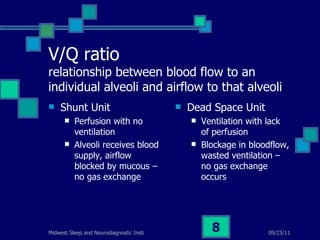
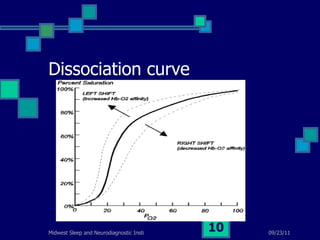
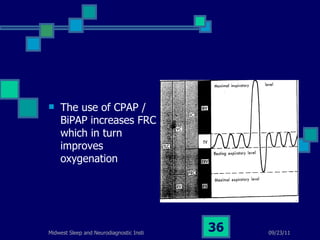
Sleep disordered breathing refers to conditions like obstructive sleep apnea that disrupt normal breathing patterns during sleep. Key factors that influence gas exchange in the lungs include the V/Q ratio and the oxygen dissociation curve. Treatment options for obstructive sleep apnea include CPAP/BiPAP devices, oral appliances, and surgeries like uvulopalatopharyngoplasty. Capnography and end-tidal carbon dioxide measurements provide important windows into a patient's ventilation.





































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)











![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)






