Downloaded 14 times
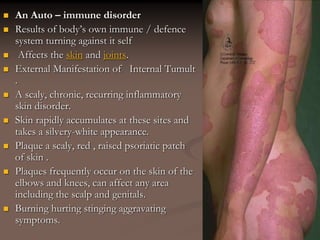
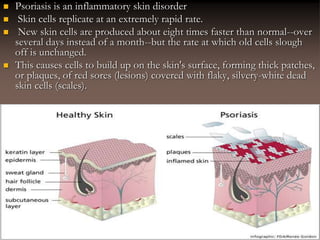



Psoriasis is a chronic, autoimmune skin disorder causing rapid skin cell growth, resulting in scaly plaques primarily on the elbows and knees, but it can affect any body area including joints (psoriatic arthritis). The disease varies in severity and can be triggered by factors such as stress, alcohol, and certain medications, impacting quality of life. Treatment options include topical treatments, phototherapy, and systemic therapies aimed at reducing symptoms and managing flare-ups.























































































