
Downloaded 266 times






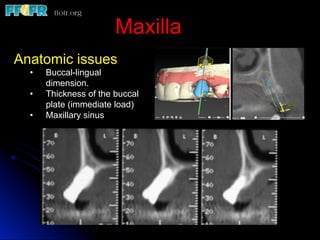














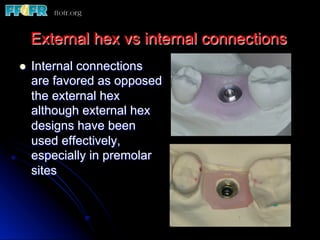

































This document discusses single tooth defects in the posterior quadrants and their restoration. It compares fixed dental prostheses to implants, noting that implants are generally preferred when adjacent teeth are healthy or nearly so. For endodontically treated teeth, a fixed restoration is preferred if sufficient tooth structure remains and occlusion and parafunction are minimal. Considerations for implant placement include anatomic factors, timing of placement, and prosthodontic issues like abutment selection and cement versus screw retention. The goal is to restore function while avoiding complications like fracture, overload, and peri-implantitis.
































































































