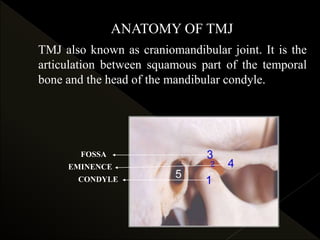
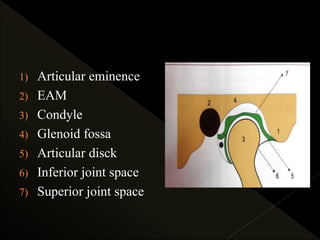
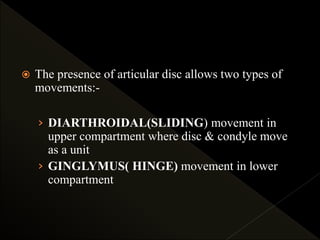
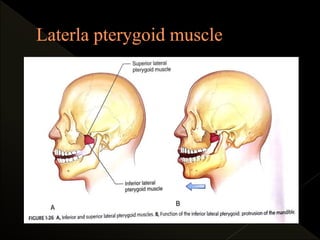
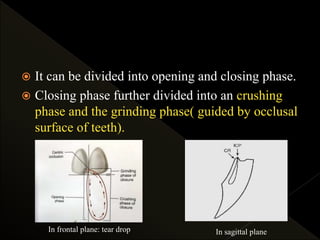

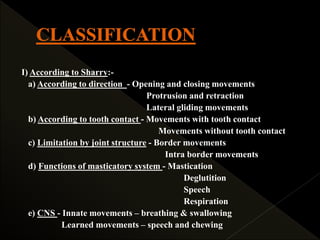
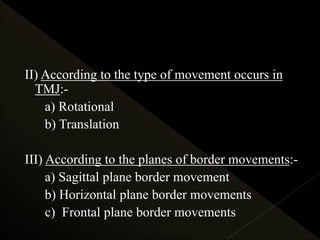
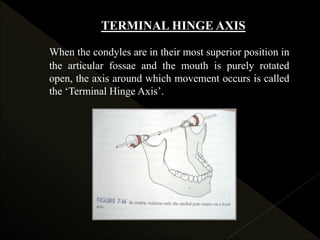
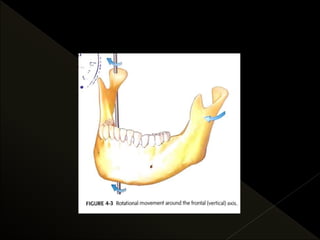
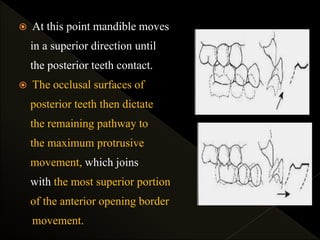
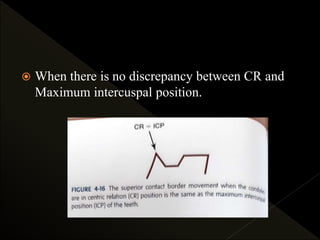
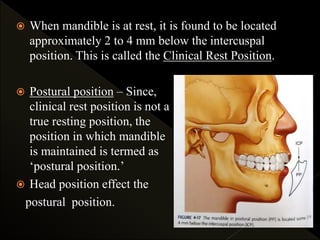


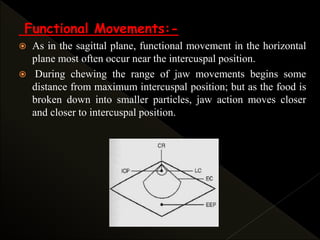
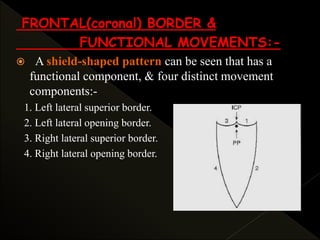
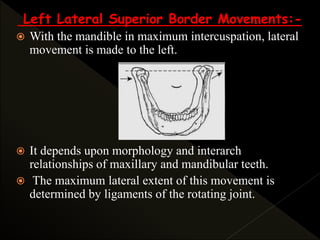
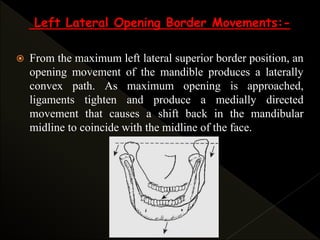
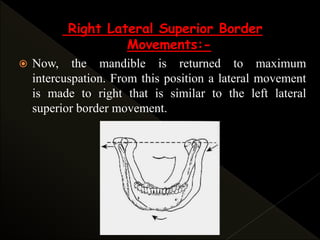
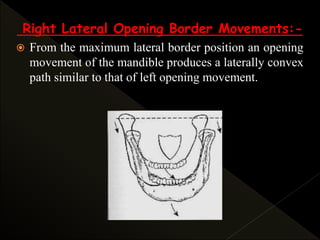
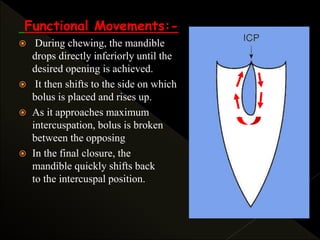

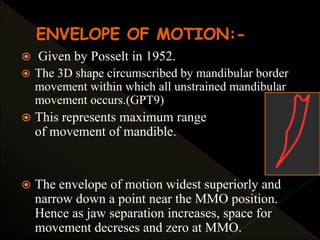
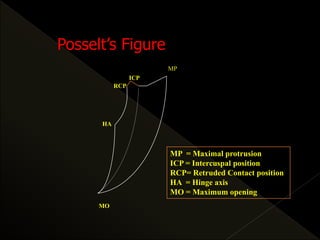

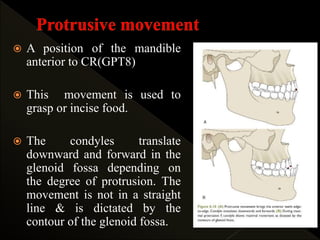
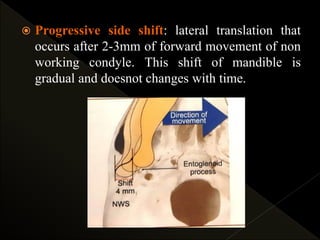
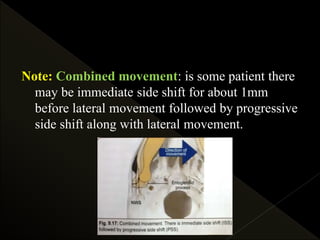
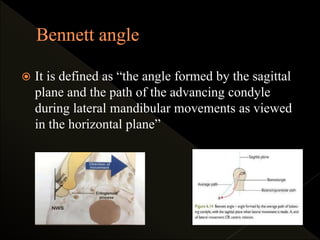


This document provides an overview of mandibular movements and the temporomandibular joint (TMJ). It discusses the anatomy of the TMJ, types of mandibular movements including rotation and translation, and the three planes of border movements: sagittal, frontal, and horizontal. It also examines the determinants of mandibular movement, including condylar guidance, anterior guidance, and the neuromuscular system. The chewing stroke and neuromuscular regulation of movement are described.



































































