
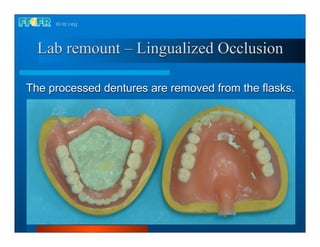
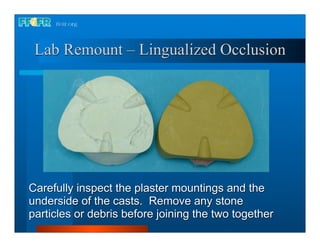
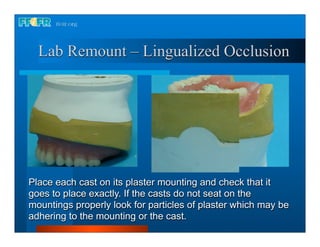
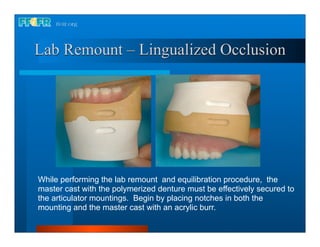
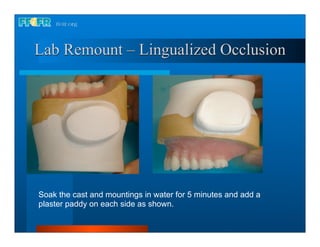
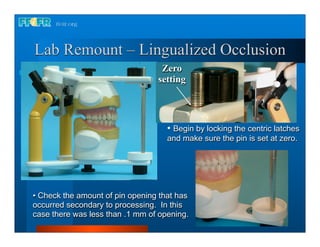
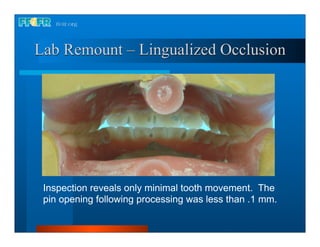
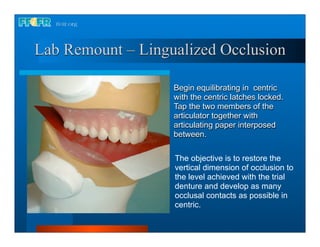
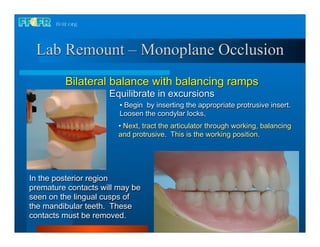
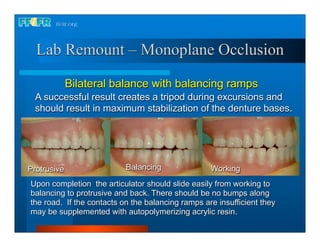
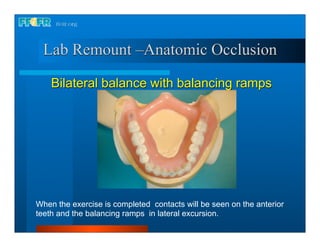
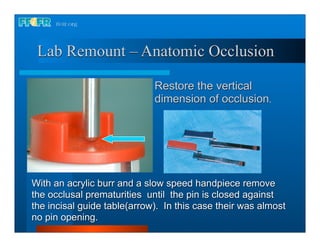
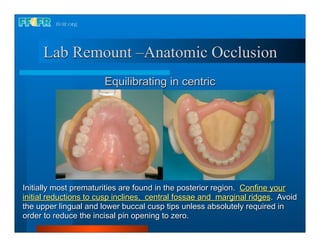
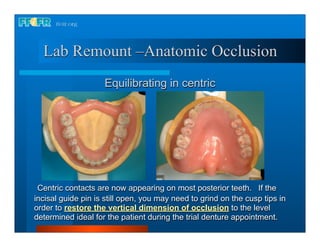
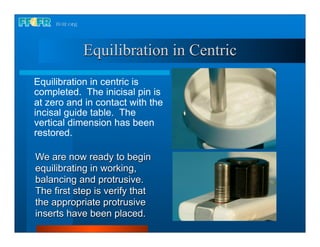
1. The document describes the process of laboratory remount, which involves correcting errors in occlusion that occurred during denture processing and restoring the correct vertical dimension and balanced occlusion. 2. Key steps include securing the dentures to articulator mounts, checking for changes in vertical dimension, equilibrating contacts in centric occlusion, and then excursions including working, balancing, and protrusive movements. 3. The goal is to develop simultaneous and balanced occlusal contacts throughout function using techniques like selective grinding of cusp inclines and fossae.
































































































