Download as PDF, PPTX



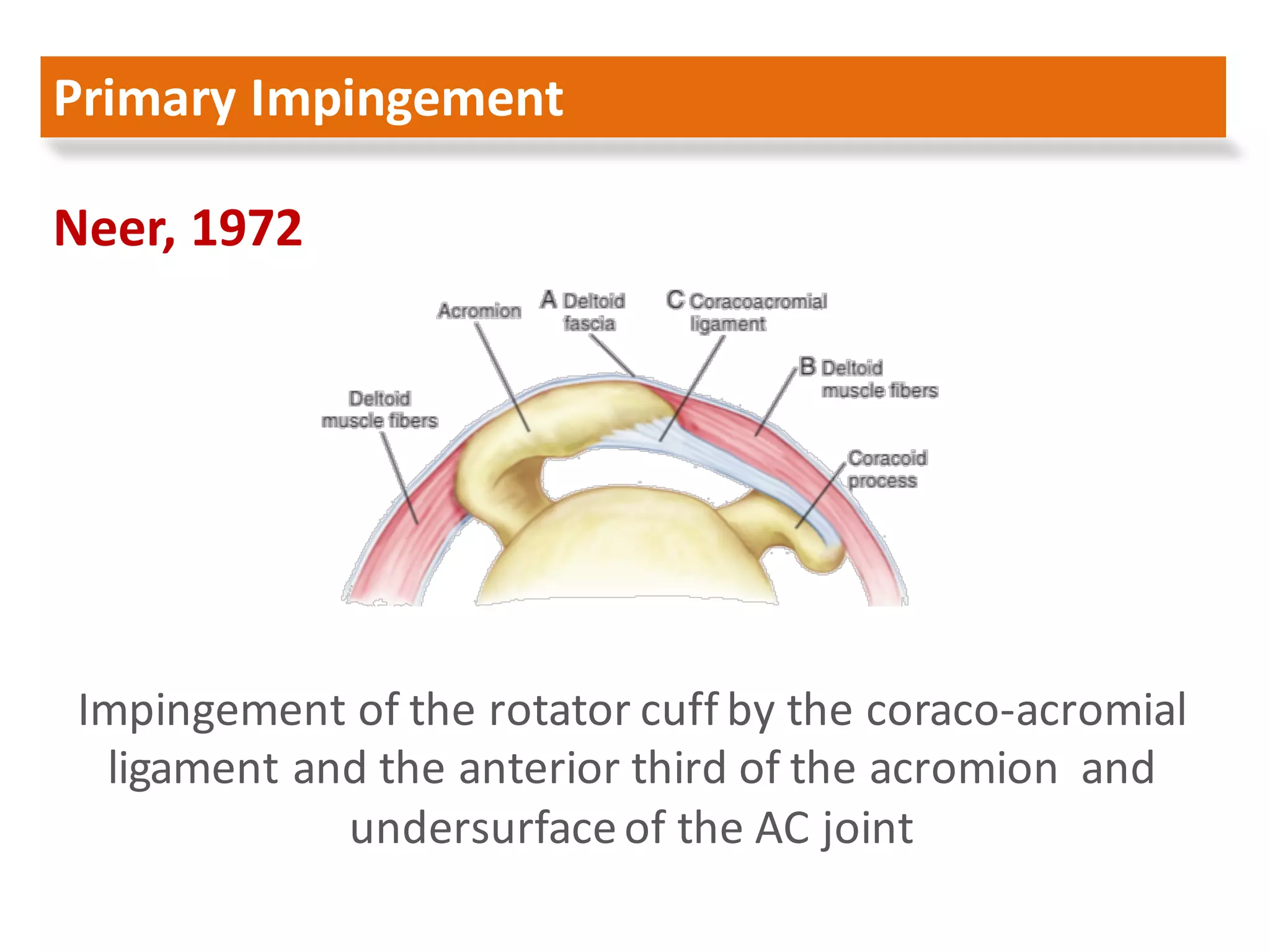










































This document provides an overview of subacromial impingement syndrome and subacromial decompression surgery. It discusses the etiology of impingement, including extrinsic factors like outlet stenosis and intrinsic factors like rotator cuff degeneration. It reviews the history and techniques of arthroscopic subacromial decompression surgery, including bursectomy, acromioplasty, and potential distal clavicle resection. Long-term studies on the efficacy of decompression are presented, with varying results on outcomes and re-tear rates.