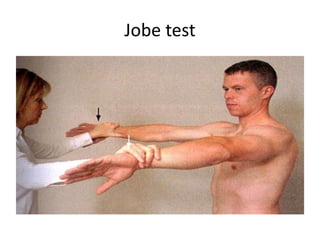
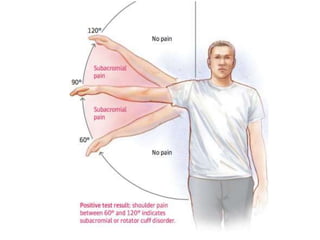
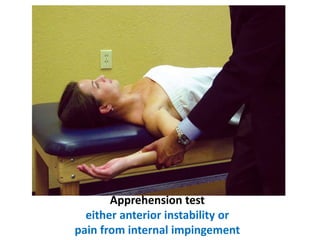
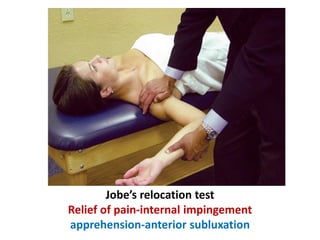
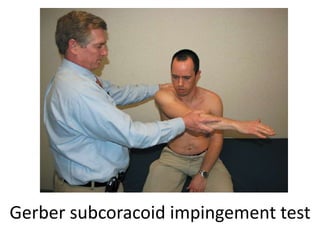
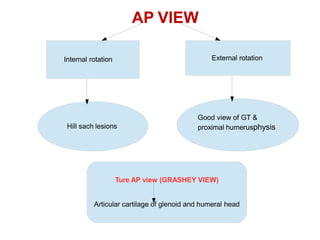
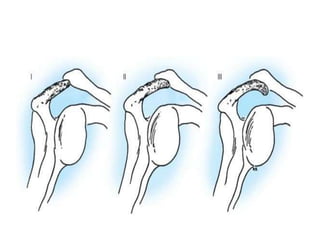
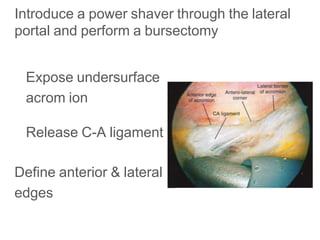
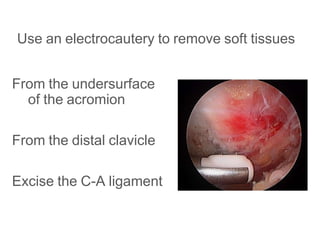
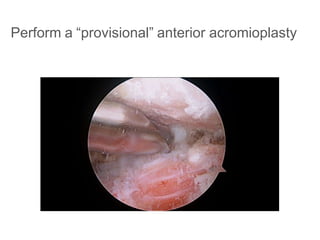
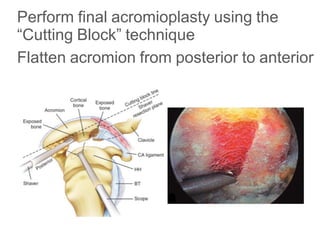
This document discusses shoulder impingement syndrome, including its history, presentation, diagnostic evaluation, and treatment. It notes that impingement was first described in 1867 and variously characterized in the early 20th century. In 1972, Neer described impingement syndrome and characterized it as being caused by repeated impingement between the rotator cuff/humeral head and acromion. The document outlines the stages of impingement syndrome and types of impingement. It discusses physical exam findings and imaging workup, and notes that treatment involves a trial of conservative measures followed by arthroscopic acromioplasty if unsuccessful.