
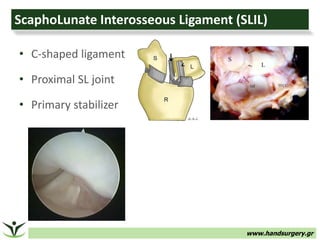
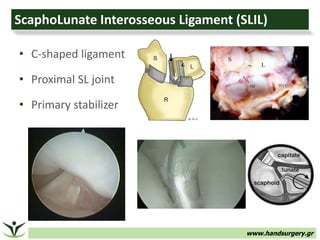
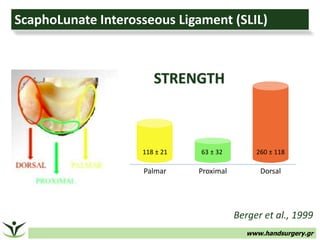
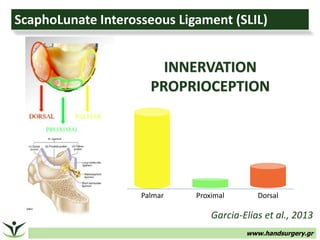
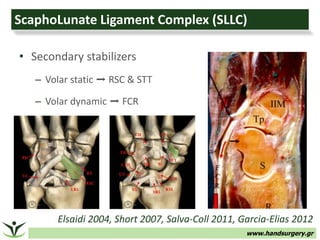
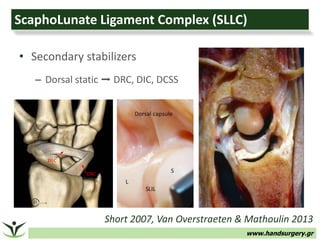
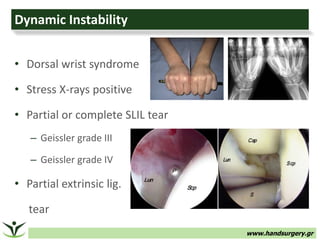
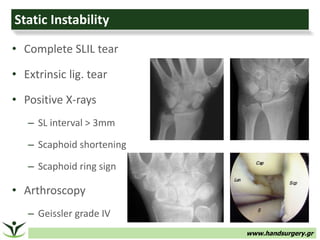
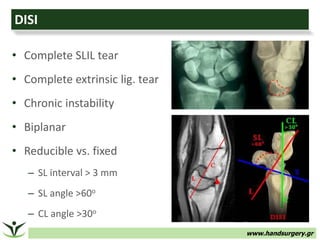
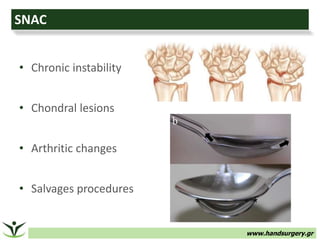
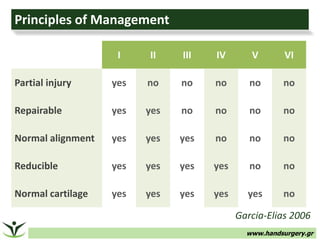

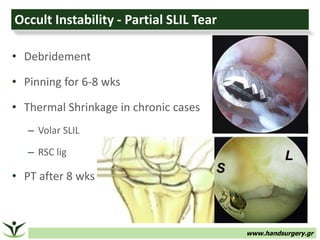
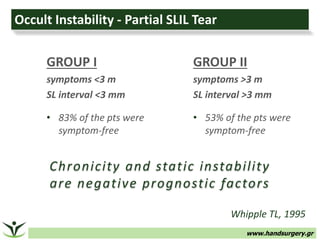
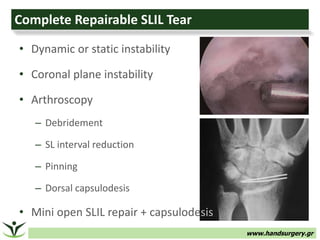

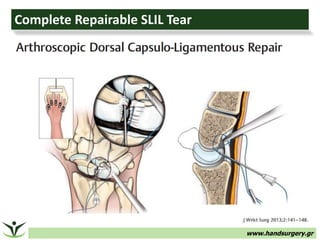
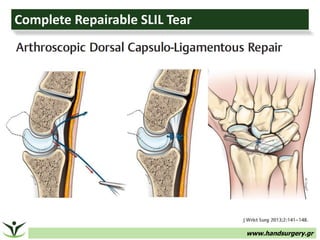
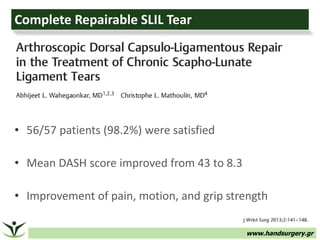

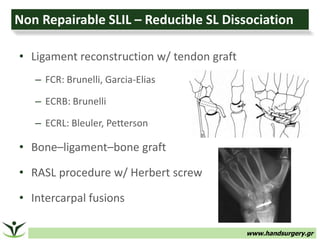
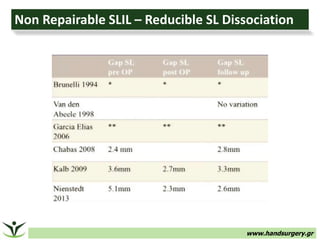
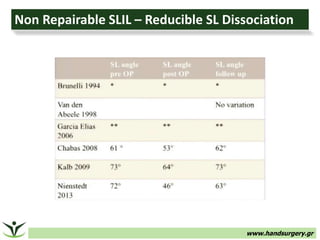
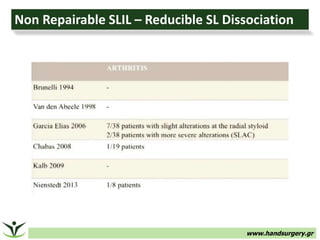
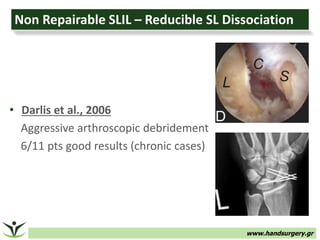



The document discusses scapholunate tears, noting that the scapholunate interosseous ligament (SLIL) is the primary stabilizer of the scapholunate joint. It describes the spectrum of injury from partial to complete tears and the importance of early diagnosis. The principles of management involve determining if the dorsal SL ligament is intact and repairable, and if carpal malalignment is reducible. Treatment options range from arthroscopic debridement for partial tears to open repair and reconstruction for complete tears.


























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

















