Download to read offline

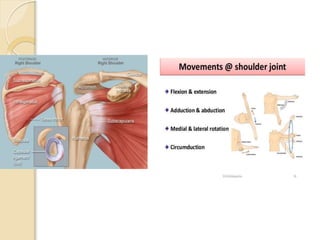







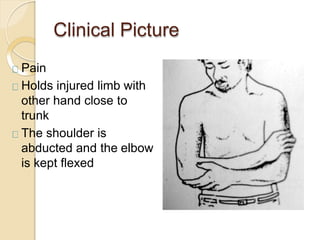



































The presentation discusses shoulder dislocation, focusing on the anatomy of the shoulder joint and the three types of shoulder dislocations: anterior, posterior, and inferior. It outlines the causes, clinical features, management strategies, and complications associated with each type. Emphasis is placed on the importance of timely reduction to prevent complications such as avascular necrosis and the management of recurrent instability.











































































