- Shoulder dislocation involves the head of the humerus becoming displaced from the glenoid cavity. Anterior dislocation is more common than posterior.
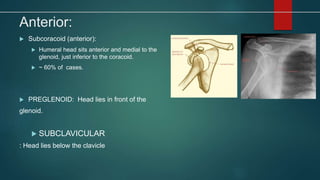
- Mechanisms include indirect falls on an outstretched arm or direct blows to the shoulder. Anterior dislocations are further classified by the position of the humeral head.
- Clinical features include pain, guarding the arm close to the body, loss of normal shoulder contour, and inability to touch the opposite shoulder.
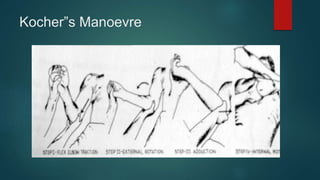
- Treatment involves closed reduction under sedation or anesthesia followed by immobilization, with later exercises to regain range of motion. Complications can include nerve injuries, recurrent dislocations, or bone defects that contribute to instability.