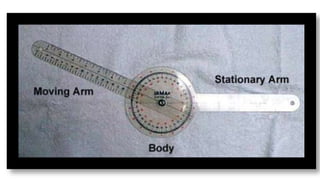
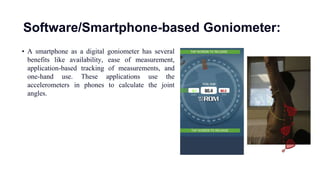
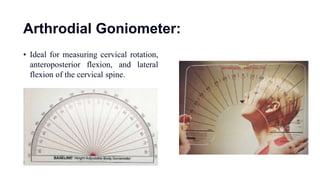
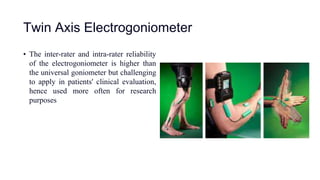
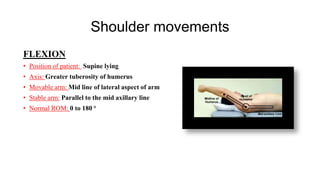
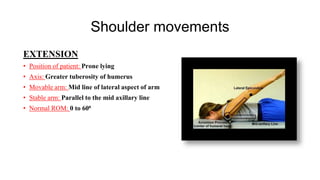
The document outlines the use of goniometry for measuring joint range of motion, primarily in the upper limbs. It details various types of goniometers, measurement procedures, and specific protocols for assessing the shoulder, elbow, and wrist movements, including normal ranges of motion. The text serves as a practical guide for physical therapists to accurately measure and track joint mobility in patients.