Downloaded 67 times










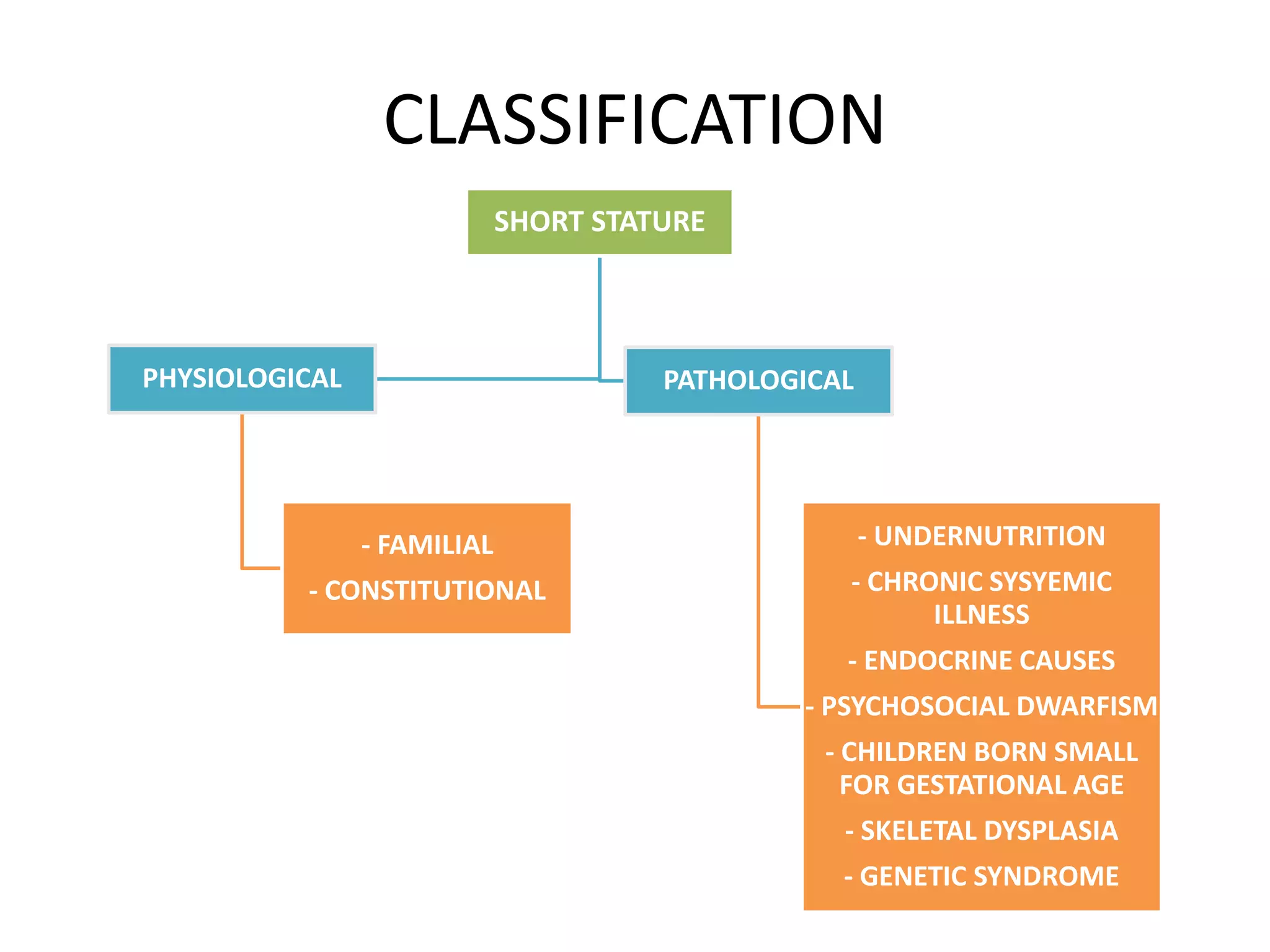














































This document provides information on short stature, including defining it as height below the third centile or more than 2 standard deviations below the median height for age and gender. It discusses assessing short stature by accurately measuring height, assessing height velocity, comparing to population norms and genetic potential. It also classifies short stature and discusses differential diagnosis, management, and approaching a case scenario.























































































