Downloaded 51 times

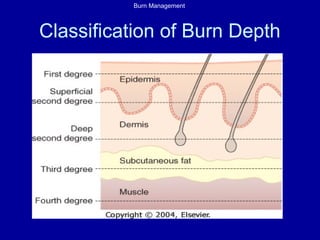

This document provides an overview of burn management, including the pathophysiology of burns, classification of burn depth, criteria for transfer to a burn center, initial assessment and management, airway management, shock and fluid resuscitation, burn wound management including for electrical and chemical burns. It details the Parkland formula for fluid resuscitation and management of potential airway compromise, circumferential limb burns requiring escharotomy, wound infection prevention and timing of excision and grafting.























































































