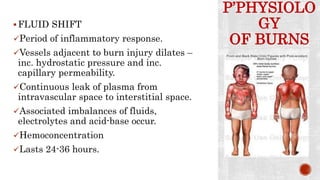
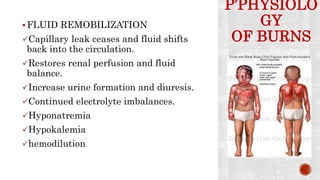
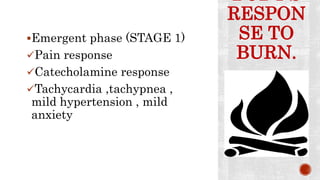
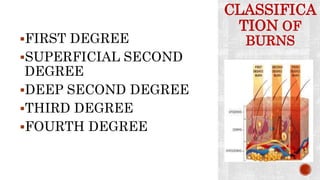
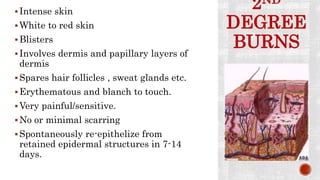
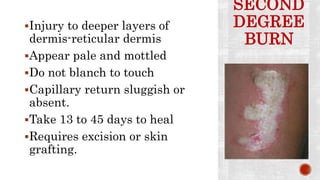
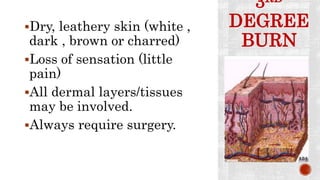
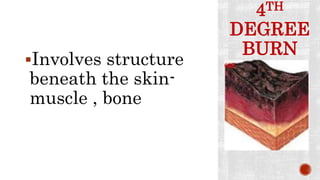
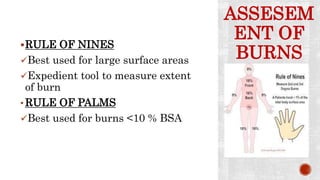
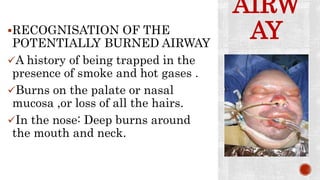
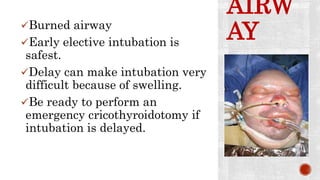
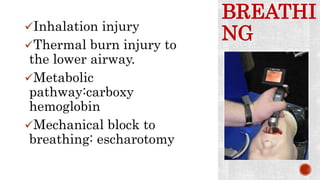
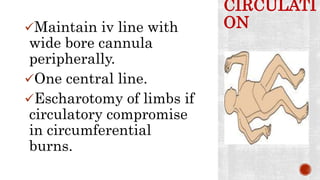
The document discusses different types of burns including thermal, chemical, electrical, and radiation burns. It describes the pathophysiology of burns including the fluid shift phase and hypermetabolic phase. Burns are classified based on depth from first to fourth degree. Management involves airway control, breathing support, fluid resuscitation, infection monitoring and control, topical treatments, and dressing selection based on burn depth.