• Definitions
• Stepsin interceptive orthodontics
• Serial extraction
• Muscle exercises
• Removal of soft / hard tissue barriers
• Management of ectopic eruption
• Management of missing permanent teeth
• Resolution of crowding
CONTENTS
3.
CONTENTS
• Correction ofmidline diastema
• Correction of developing crossbite
• Functional appliances
• Orthopedic appliances
• Maxillary intrusive splint
• Pre orthodontic trainer
• Bent wire system
• Invisalign
• Conclusion
• References.
4.
DEFINITION- AAO (1969)
•That phase of the science & art of orthodontics
employed to recognize & eliminate potential
irregularities & malpositions in the developing
dentofacial complex.
5.
“Interceptive orthodontics”basically refers to
measures undertaken to prevent a potential
malocclusion from progressing into a more severe
One.
Is undertaken at a time when the malocclusion has
already developed or still developing.
Procedures, are aimed at elimination of factors,
that may lead to malocclusion.
6.
Serial extraction
Dev. Crossbite
Abnormal habits
Space regaining
Muscle exercises
Removal of barrier-
eruption
Interceptive
Orthodontics
Interception of
skeletal
malrelation
7.
SERIAL EXTRACTION
Historical review-
Kjellgren(1929) : Serial extraction
Hotz (1970) : Guidance of eruption
Palsson & Bunon: (1743) first ref to the extraction
of deci teeth (Publication- Diseases of Teeth)
Nance (1940) : popularized the technique
Father of serial extraction
8.
SERIAL EXTRACTION
• DEFINITION:
–Dewel (1967) : orderly removal of selected primary
& permanent teeth in predetermined sequence
-Tweed : planned & sequential removal of primary
& permanent teeth to intercept & reduce dental
crowding problems
9.
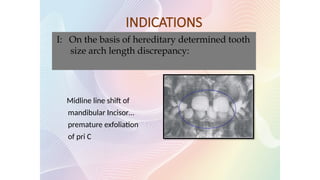
I: On thebasis of hereditary determined tooth
size arch length discrepancy:
Midline line shift of
mandibular Incisor…
premature exfoliation
of pri C
INDICATIONS
10.
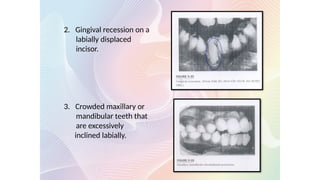
2. Gingival recessionon a
labially displaced
incisor.
3. Crowded maxillary or
mandibular teeth that
are excessively
inclined labially.
11.
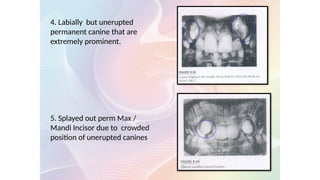
4. Labially butunerupted
permanent canine that are
extremely prominent.
5. Splayed out perm Max /
Mandi Incisor due to crowded
position of unerupted canines
12.
6. Unusual shape,size and no of teeth.
7. Ectopic eruption of maxillary 1st molar
8. Premature loss of primary canine
9. Abnormal / pathological root resorption of primary canine.
10. Crowded anteriors
13.
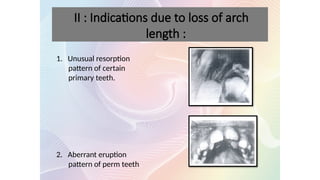
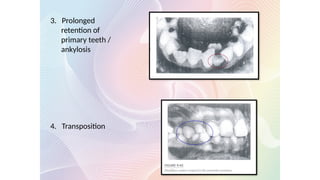
1. Unusual resorption
patternof certain
primary teeth.
2. Aberrant eruption
pattern of perm teeth
II : Indications due to loss of arch
length :
CONTRAINDICATIONS
1. Skeletal ClassII and Class III malformation.
2. Spaced dentitions
3. Anodontia / oligodontia
4. Open bite & deep bite
5. Midline diastema
6. Class I malocclusions with minimal space def.
7. Unerupted malformed teeth Eg: dilacerations
8. Mild disproportions b /w arch length & tooth material
that can be treated by proximal stripping.
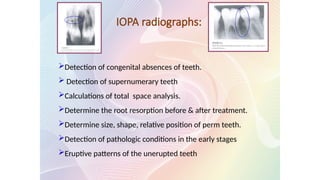
IOPA radiographs:
Detection ofcongenital absences of teeth.
Detection of supernumerary teeth
Calculations of total space analysis.
Determine the root resorption before & after treatment.
Determine size, shape, relative position of perm teeth.
Detection of pathologic conditions in the early stages
Eruptive patterns of the unerupted teeth
19.
Cephalometric radiographs:
Evaluationof craniofacial relationship before treatment
Assessment of soft tissue matrix.
Classification of facial patterns.
Calculation of tooth –size / jaw- size discrepancies.
Prediction of growth & development
Detection pathologic conditions before, during and after treatment.
Determination of mandibular rest positions
20.
Facial photographs
Evaluationof craniofacial (&dental) relationships& proportions
before treatment.
Assessment of soft tissue profile.
Proportional facial analysis & Total space analysis
Monitoring treatment progress.
Study relationships before, immediately following & several years
treatment.
Detecting & recording facial asymmetry.
Identifying patients
Intra oral photographs
21.
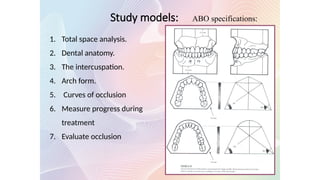
1. Total spaceanalysis.
2. Dental anatomy.
3. The intercuspation.
4. Arch form.
5. Curves of occlusion
6. Measure progress during
treatment
7. Evaluate occlusion
ABO specifications:
Study models:
22.
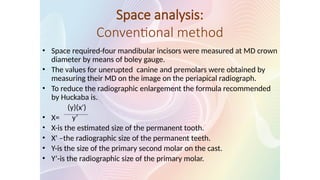
Space analysis:
Conventional method
•Space required-four mandibular incisors were measured at MD crown
diameter by means of boley gauge.
• The values for unerupted canine and premolars were obtained by
measuring their MD on the image on the periapical radiograph.
• To reduce the radiographic enlargement the formula recommended
by Huckaba is.
(y)(x')
• X= y’
• X-is the estimated size of the permanent tooth.
• X’ –the radiographic size of the permanent teeth.
• Y-is the size of the primary second molar on the cast.
• Y’-is the radiographic size of the primary molar.
23.
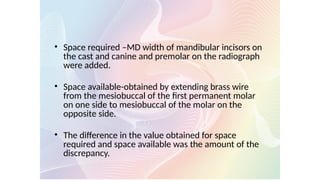
• Space required–MD width of mandibular incisors on
the cast and canine and premolar on the radiograph
were added.
• Space available-obtained by extending brass wire
from the mesiobuccal of the first permanent molar
on one side to mesiobuccal of the molar on the
opposite side.
• The difference in the value obtained for space
required and space available was the amount of the
discrepancy.
24.
ADVANTAGES OF SERIAL
EXTRACTION
Removal of deciduous canines….
Extraction of deciduous 1st
molar….
Extraction of first premolar before crowding allows…
It lessens the period of future appliance therapy and
cost of treatment.
25.
ADVERSE EFFECTS
First (Dewel-1967),tendency of developing
anterior deep bite following loss of posterior teeth.
Second side effect is failure of premolars to reach their normal
occlusal level.
Third : Effect of Serial Extraction has on facial esthetics.
The over emphasis on straight profile…..
Lip fullness is not a reliable criterion
The straight profile must be viewed with greater concern
because early removal of premolars…
26.
Fourth : Nasaldevelopment is another unpredictable hazard
Unrestrained extraction will accentuate nose prominence
by reducing skeletal development in dental area.
Moreover growth of chin is unpredictable. If growth in nose
and chin exceeds normal range a concave profile is
obtained.
27.
Most common &accepted
sequences:-
1. Tweed’s method
2. Dewel’s methd
3. Nance’s method
4. Grewe’s method
28.
Dewel’s Method: 1978(CD4)
– There are 3 stages in Serial Extraction Therapy:
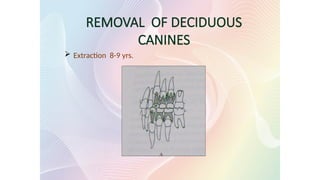
• Removal of deciduous canines:
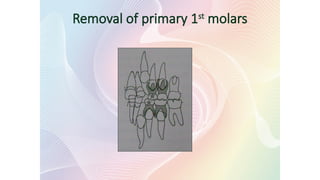
• Removal of first deciduous molars:
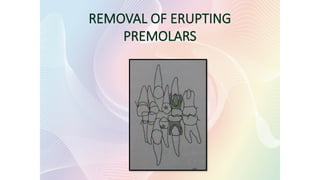
• Removal of erupting premolars:
TWEED’S SEQUENCE OF
EXTRACTION(1966)
• Sequence is :DC4
– At approx 8 years all deci 1st molars are extracted.
– Deciduous canines maintained to retard eruption of
permanent canines.
– 1st premolar –in advanced eruptive stage- crown above alv
bone.
– Deciduous canines along with first premolar are extracted
33.
Treatment procedure inclass I
malocclusion
Group A - Anterior discrepancy : crowding
Group B - Anterior discrepancy : Alveolodental protrusion
Group C - Middle discrepancy : impacted canine
Group D - Enucleation in mandible
Group E - Enucleation in mandible & maxilla
Group F - Alternative to enucleation
Group G - Interproximal stripping
Group H- congenital absence
34.
Closure ofResidual Xn spaces
Improvement in axial inclination
Correction of rotation
Correction of Midline discrepancy
Correction of residual overbite and overjet
Correction of cross bites
Improvement in arch form
Advantages of mechanotherapy
35.
MUSCLE EXERCISES
Thedental tissues are blanketed from all directions
by the muscles
Normal occlusal development depends on normal
oro-facial muscle function.
Muscle exercises helps in improving aberrant muscle
function.
36.
1. Exercise forthe masseter muscle:
2. Exercise for the lips:
Stretching of upper lip to maintain lip seal for
short hypotonic lips
Holding a piece of paper between lips
Holding and pumping of water back and forth
behind the lips.
Massaging of lips
Scotch tape
Button pull exercise:
37.
3. Exercise forthe pterygoid muscles:
4. Exercise for the tongue: (5/16 inch intra oral elastic)
One elastic swallow:
Tongue hold exercise:
Two elastic swallow:
The hold pull exercise: tongue tie exercise
38.
Limitation of muscleexercises
• Does not drastically alter any growth pattern
• Are not substitute for corrective orthodontic
treatment
• Pt compliance is extremely important
39.
• Retained deciduousteeth
• Supernumerary teeth
• Fibrous/ Bony obstruction of the erupting
tooth bud
• Impacted teeth
REMOVAL OF SOFT /HARD TISSUE BARRIERS IN
THE PATHWAY OF ERUPTION
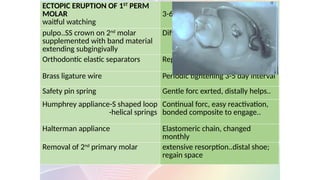
ECTOPIC ERUPTION OF1ST
PERM
MOLAR
waitful watching
3-6 month
pulpo..SS crown on 2nd
molar
supplemented with band material
extending subgingivally
Difficult to do
Orthodontic elastic separators Replacement at 1-2wks..2mnths
Brass ligature wire Periodic tightening 3-5 day interval
Safety pin spring Gentle forc exrted, distally helps..
Humphrey appliance-S shaped loop
-helical springs
Continual forc, easy reactivation,
bonded composite to engage..
Halterman appliance Elastomeric chain, changed
monthly
Removal of 2nd
primary molar extensive resorption..distal shoe;
regain space
42.
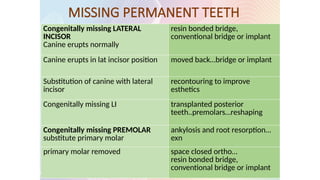
Management: arch length,adjacent tooth morphology and
colour,incisor position and esthetics
MISSING PERMANENT TEETH
Congenitally missing LATERAL
INCISOR
Canine erupts normally
resin bonded bridge,
conventional bridge or implant
Canine erupts in lat incisor position moved back…bridge or implant
Substitution of canine with lateral
incisor
recontouring to improve
esthetics
Congenitally missing LI transplanted posterior
teeth..premolars…reshaping
Congenitally missing PREMOLAR
substitute primary molar
ankylosis and root resorption…
exn
primary molar removed space closed ortho…
resin bonded bridge,
conventional bridge or implant
43.
Resolution of crowding
Anteriorsegment- incisal liability
Posterior segment- leeway space of nance
Management:
1. Observation
2. Disking of primary teeth-hand held strip, tapered bur in a high
speed handpiece
3. Extractions and serialextraction
4. Corrective orthodontic referral
44.
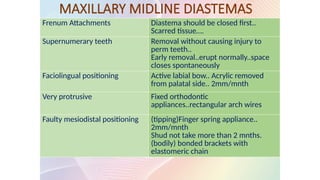
MAXILLARY MIDLINE DIASTEMAS
FrenumAttachments Diastema should be closed first..
Scarred tissue….
Supernumerary teeth Removal without causing injury to
perm teeth..
Early removal..erupt normally..space
closes spontaneously
Faciolingual positioning Active labial bow.. Acrylic removed
from palatal side.. 2mm/mnth
Very protrusive Fixed orthodontic
appliances..rectangular arch wires
Faulty mesiodistal positioning (tipping)Finger spring appliance..
2mm/mnth
Shud not take more than 2 mnths.
(bodily) bonded brackets with
elastomeric chain
45.
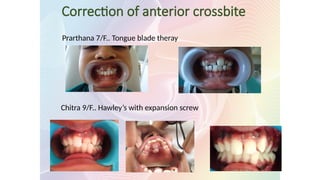
Correction of developingAnterior
and Posterior Cross Bites
• Eliminates functional shifts and wear on the erupted permanent teeth
• Dentoalveolar asymmetry
• Increases circumference and provides more room for permanent teeth
47.
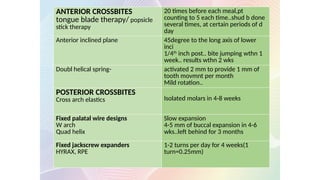
ANTERIOR CROSSBITES
tongue bladetherapy/ popsicle
stick therapy
20 times before each meal,pt
counting to 5 each time..shud b done
several times, at certain periods of d
day
Anterior inclined plane 45degree to the long axis of lower
inci
1/4th
inch post.. bite jumping wthn 1
week.. results wthn 2 wks
Doubl helical spring- activated 2 mm to provide 1 mm of
tooth movmnt per month
Mild rotation..
POSTERIOR CROSSBITES
Cross arch elastics Isolated molars in 4-8 weeks
Fixed palatal wire designs
W arch
Quad helix
Slow expansion
4-5 mm of buccal expansion in 4-6
wks..left behind for 3 months
Fixed jackscrew expanders
HYRAX, RPE
1-2 turns per day for 4 weeks(1
turn=0.25mm)
48.
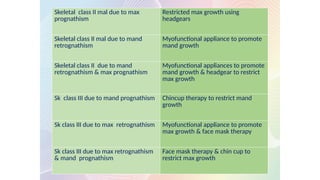
INTERCEPTION OF SKELETAL
MALOCCLUSION
Skeletalclass II mal due to max
prognathism
Restricted max growth using
headgears
Skeletal class II mal due to mand
retrognathism
Myofunctional appliance to promote
mand growth
Skeletal class II due to mand
retrognathism & max prognathism
Myofunctional appliances to promote
mand growth & headgear to restrict
max growth
Sk class III due to mand prognathism Chincup therapy to restrict mand
growth
Sk class III due to max retrognathism Myofunctional appliance to promote
max growth & face mask therapy
Sk class III due to max retrognathism
& mand prognathism
Face mask therapy & chin cup to
restrict max growth
49.
FUNCTIONAL APPLIANCES
• Myofunctionalappliances - harness the muscle
pressure
• Functional appliances- elicit certain natural
functions of the orofacial region
50.
• Functional appliancesare conceptually based
on Moss’ functional matrix theory
Form follows function
BACKGROUND
51.
These applianceseither transmit, eliminate or
guide the natural forces of the masculature.
Are used for growth modification procedures that
are aimed at intercepting and treating jaw
discrepancies
They bring about following changes:
An increase or decrease in jaw size.
A change in spatial relationship of the jaws
Change in direction of growth of the jaws
Acceleration of desirable growth
52.
classifications
I) Tom Graber,when functionals were removable:
Group A- teeth supported appliances eg.
Catalans, inclined planes, etc.
Group b- teeth/tissues supported appliances.
Eg. Activator, bionator, etc.
Group c- vestibular positioned appliances.
With isolated support from tooth / tissue eg. Oral
Screens, frankel, lip bumpers.
53.
classification
II) With theadvent of fixed functionals another classification
evolved:
A)Removable functionals eg. Activator, Frankel etc.
B)semi fixed functionals eg. Den holtz, Bass appliances.
C)fixed functionals eg. Herbst, Jasper jumper, MARA, etc.
54.
classification
III) With theawareness & acceptance of the concept of
hybridism by Peter Vig, functionals could be further
classified as
A)classic functional appliances like
Activator, Catalans, Frankel etc.
B)hybrid appliances like Propulsor, Double Oral
screen, Hybrid bionators, bass appliance.
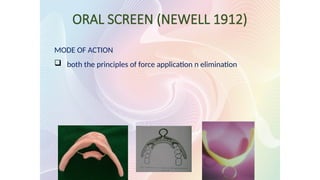
ORAL SCREEN (NEWELL1912)
MODE OF ACTION
both the principles of force application n elimination
57.
Indications :
Interceptionof habits like –
Correction of mild disto-occlusion
Muscle exercises for correction of hypotonic lip & cheek
muscles.
Correction of mild anterior proclination.
Fabrication :
Impression
Sealing of cast in occlusion
Covering of labial surfaces of teeth & alveolar process with
wax of 2-3mm thickness.
Fabrication of appliance with self cure or heat cure resin.
Patient is asked to wear the appliance in the night & 2-3 hrs
during the day time.
Seen about once every 3 weeks or a month
58.
Modification of vestibularscreen
1. Hotz modification- metal ring- muscle
exercises
2. Double oral screen- tongue thrust
3. With holes- mouth breathers
59.
LIP BUMPER
• Combinedremovable fixed appliance
• Muscular force application or force elimination
• Both maxilla and mandible
• USES:
o Lip sucking
o Hyperactive mentalis- crowding of lower ant
o Distalization of first molars
Maxillary arch- Denholtz appliance
ACTIVATOR
Kingsley 1879 :Vulcanite palatal plate.
Hotz : Vorbissplate
Perrie Robin- Monoblock
Viggo Andreasen 1908 :Biomechanical working retainer
Along with Karl Haulp - Norwegian appliance
It was named activator because of its ability to activate
muscle forces.
62.
MODE OF ACTION
1.Myotactic reflex- Introduces a new pattern of mandibular
closure
2. Condylar adaptation- Backward & upward growth
3. Force generated while swallowing & sleep
INDICATIONS:
Class II, div 1 malocclusion.
Class II, div 2
Class III malocclusion
Class I, open bite
Class I, deep bite
Post treatment retention.
Children with decreased lower facial height.
63.
Fabrication of appliance
•Impression
• Bite registration
• Articulation of the model
• Preparation of wire element- labial bow-0.8 or
0.9mm wire
• Fabrication of acrylic portion
o Maxillary part
o Mandibular part
o Interocclusal part
Trimming of theactivator
• For vertical control
Intrusion of teeth-
Extrusion of teeth-
66.
• For sagittalcontrol
Class II correction
Protrusion & retrusion of incisors
67.
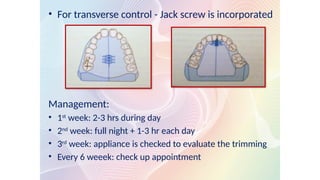
• For transversecontrol - Jack screw is incorporated
Management:
• 1st
week: 2-3 hrs during day
• 2nd
week: full night + 1-3 hr each day
• 3rd
week: appliance is checked to evaluate the trimming
• Every 6 weeek: check up appointment
68.
MODIFICATIONS
• Bow activatorof Schwarz
• Wunderer’s modification
• Propulsor
• Reduced activator or cybernator of Schmuth
• Cutout or palate free activator
• Karwetzky modification
• Herren’s modification
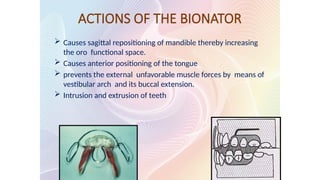
ACTIONS OF THEBIONATOR
Causes sagittal repositioning of mandible thereby increasing
the oro functional space.
Causes anterior positioning of the tongue
prevents the external unfavorable muscle forces by means of
vestibular arch and its buccal extension.
Intrusion and extrusion of teeth
72.
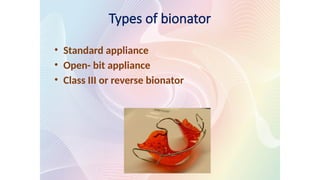
Types of bionator
•Standard appliance
• Open- bit appliance
• Class III or reverse bionator
73.
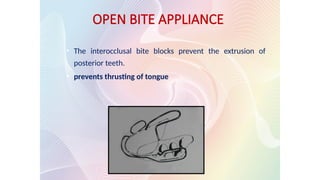
OPEN BITE APPLIANCE
•The interocclusal bite blocks prevent the extrusion of
posterior teeth.
• prevents thrusting of tongue
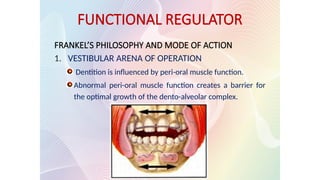
FUNCTIONAL REGULATOR
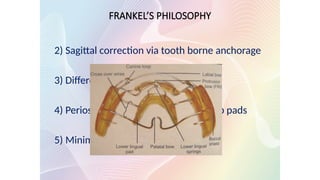
FRANKEL’S PHILOSOPHYAND MODE OF ACTION
1. VESTIBULAR ARENA OF OPERATION
Dentition is influenced by peri-oral muscle function.
Abnormal peri-oral muscle function creates a barrier for
the optimal growth of the dento-alveolar complex.
• Frankel-Ia
– classI malocclusion, minor to moderate crowding & deep
bite cases.
• Frankel-Ib
– class II, division 1 malocclusion
– overjet < 7mm.
Types of Frankel appliances
78.
• Frankel-Ic
– Cl- II division 1 malocclusion
– overjet >7mm.
• Frankel-II
– CL-II and division 1 & 2
– Is modified by adding a stainless
steel protrusion bow behind the
maxillary incisors.
Types of Frankel appliances
79.
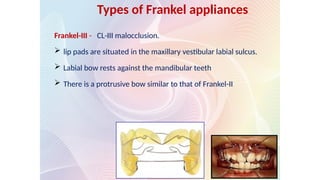
Frankel-III - CL-IIImalocclusion.
lip pads are situated in the maxillary vestibular labial sulcus.
Labial bow rests against the mandibular teeth
There is a protrusive bow similar to that of Frankel-II
Types of Frankel appliances
80.
FRANKEL-IV
correction ofopen bite & to a lesser extent in
bimaxillary protrusion.
redirect the mandibular growth from a downward &
backward growth rotation to a upper and forward
rotation.
Frankle V
• Used along with headgears
81.
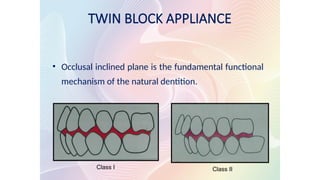
TWIN BLOCK APPLIANCE
•Occlusal inclined plane is the fundamental functional
mechanism of the natural dentition.
Class I Class II
82.
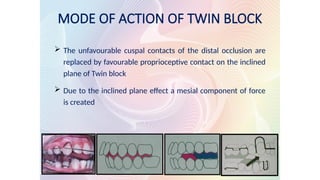
MODE OF ACTIONOF TWIN BLOCK
The unfavourable cuspal contacts of the distal occlusion are
replaced by favourable proprioceptive contact on the inclined
plane of Twin block
Due to the inclined plane effect a mesial component of force
is created
83.
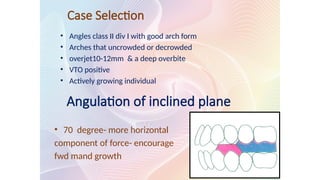
Case Selection
• Anglesclass II div I with good arch form
• Arches that uncrowded or decrowded
• overjet10-12mm & a deep overbite
• VTO positive
• Actively growing individual
Angulation of inclined plane
• 70 degree- more horizontal
component of force- encourage
fwd mand growth
84.
Stages of treatment
•Active phase – 6-9 months
• Support phase- 3-6 months
• Retention phase- 9 months
• avg- 18 months
• 8-10 hours a day
• 2-3 months
85.
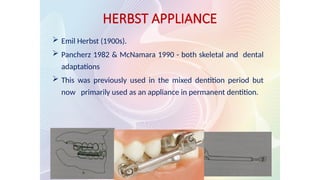
Emil Herbst(1900s).
Pancherz 1982 & McNamara 1990 - both skeletal and dental
adaptations
This was previously used in the mixed dentition period but
now primarily used as an appliance in permanent dentition.
HERBST APPLIANCE
86.
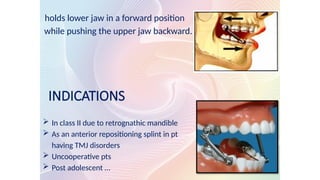
holds lower jawin a forward position
while pushing the upper jaw backward.
INDICATIONS
In class II due to retrognathic mandible
As an anterior repositioning splint in pt
having TMJ disorders
Uncooperative pts
Post adolescent …
87.
TREATMENT EFFECTS
ClassII to class I molar relation
Increase in mand growth
Distal driving of max molars
Overjet reduction
An inhibitory influence on sagittal max growth
88.
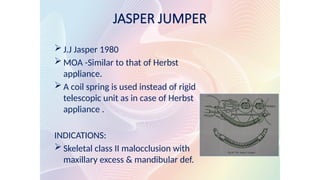
JASPER JUMPER
J.JJasper 1980
MOA -Similar to that of Herbst
appliance.
A coil spring is used instead of rigid
telescopic unit as in case of Herbst
appliance .
INDICATIONS:
Skeletal class II malocclusion with
maxillary excess & mandibular def.
89.
Acc Sassouni etal- 1972
• Orthodontic therapy- aimed at correction of
dentoalveolar malocclusion
• Orthopedic therapy- correction skeletal imbalance
with correction of any dentoalveolar malocclusion
being of less importance
• Orthopedic forces are heavier (400gm) when
compared to orthodontic forces( 50-100gm)
ORTHOPEDIC APPLIANCES
90.
Basis for orthopedicappliances
• Makes use of teeth as a “handle” to transmit forces
to the underlying skeletal structures.
1. Amount of force -400-600gm/side
2. Duration of force- 12-14hrs /day
3. Direction of force- posteriorly &superiorly through
the centre of resistance of the maxilla.
4. Age of the patient-
5. Timing of force application-
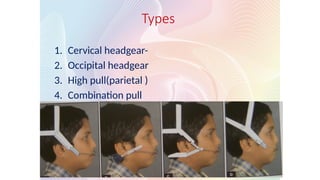
HEAD GEARS
Distalize themaxillary dentition or maxilla it self.
350 -450 gms on each side for 12-14 hrs / day.
COMPONENTS :
Force delivering unit- Face bow, J hook
Force generating unit ( elastic / springs )
Anchorage unit ( head strap/ cervical strap )
CHIN CUP THERAPY
Objective- to provide growth inhibition or redirection
& posterior positioning of mandible.
95.
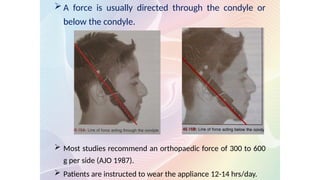
A forceis usually directed through the condyle or
below the condyle.
Most studies recommend an orthopaedic force of 300 to 600
g per side (AJO 1987).
Patients are instructed to wear the appliance 12-14 hrs/day.
96.
Ideal patient forchin cup-
Acc to T M Graber
• A mild skeletal problem with the ability to bring incisors
edge to edge or nearly so
• Short vertical facial height
• normally positioned or protrusive , but not retrusive lower
incisors
Types of chin cup
1. Occipital pull chin cup-
Classs III with mild to moderate prognathism
pt with short facial height also benefits from yhis type
2. Vetical pull chin cup- high angle cases or long face patients
97.
PROTRACTION FACE MASK
Hickham 1972.. Reverse head gear
Mainly used to pull the max ahead simultaneously pushing
the mandible distally.
250gm per side for 13 months
12-24 hrs/day.
98.
MAXILLARY INTRUSIVE SPLINT
•Indication –severe “gummy” class II div 1
malocclusion
• It reduces the visibility & vulnerability of the
maxillary incisors by
Achieving intrusion of max teeth
Restraining the max growth
Forward mandibular rotation
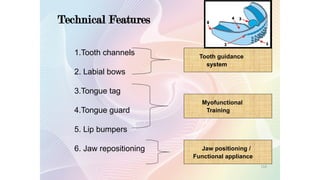
Technical Features
1.Tooth channels
2.Labial bows
3.Tongue tag
4.Tongue guard
5. Lip bumpers
6. Jaw repositioning
Tooth guidance
system
Myofunctional
Training
Jaw positioning /
Functional appliance
116
102.
Phase 1
Soft: maximum compliance & flexibility
Adapts to severe dental alignment
made of Silicone
Recommended use :
Every day for 1 hr plus overnight while
the child sleeps
Duration : 6 – 8 months
117
103.
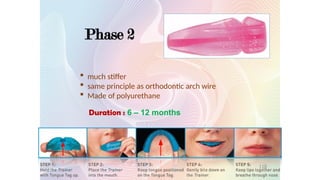
Phase 2
Duration :6 – 12 months
much stiffer
same principle as orthodontic arch wire
Made of polyurethane
118
104.
The TRAINER System™
T4K™- The Pre-orthodontic TRAINER™.Improves
facial & dental development in the growing child
(mixed dentition).
T4A™ - Aligns and retains anterior teeth in the per
manent dentition.
INFANT TRAINER™ - For habit correction.To assist
development of teeth & jaws in the growing child.
119
105.
The TRAINER System™cont’.,
T4B™ - The TRAINER for Braces.Shields the soft
tissue from brackets.
T4CII™ - The TRAINER for Class II Correction.
Jaw alignment in combination with fixed
orthodontics.
LINGUA™ - Train the Tongue Day & Night.tongue
retraining.
120
106.
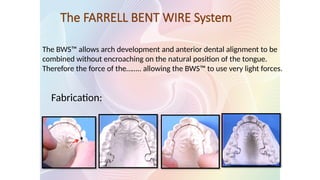
The FARRELL BENTWIRE System
The BWS™ allows arch development and anterior dental alignment to be
combined without encroaching on the natural position of the tongue.
Therefore the force of the…….. allowing the BWS™ to use very light forces.
Fabrication:
107.
Uses:
Dental arch alignment
Alongwith trainer for treatment of habits
Advantages:
Eliminate speech and functional problems
Fixed; no patient compliance
Stability..along with trainer
No lab work…..
Cost effective
Management:
Follow Up Visits Every 2 - 3 Weeks
Activation at the loops should be no more than one
millimeter initially then subsequently 1–2mm every three to four
weeks.
Open the loops bilaterally with Adams pliers at the base of the loop
and place a compensating bend……
108.
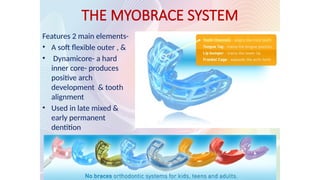
THE MYOBRACE SYSTEM
Features2 main elements-
• A soft flexible outer , &
• Dynamicore- a hard
inner core- produces
positive arch
development & tooth
alignment
• Used in late mixed &
early permanent
dentition
110.
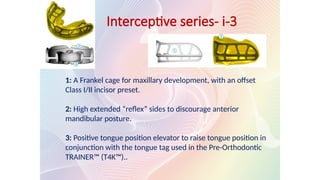
Interceptive series- i-3
1:A Frankel cage for maxillary development, with an offset
Class I/II incisor preset.
2: High extended “reflex” sides to discourage anterior
mandibular posture.
3: Positive tongue position elevator to raise tongue position in
conjunction with the tongue tag used in the Pre-Orthodontic
TRAINER™ (T4K™)..
111.
• custom-made seriesof
aligners .
• These aligner trays are made
of smooth, comfortable and
virtually invisible plastic .
• Wearing the aligners will
gradually and gently….
• You just pop in a new set of
aligners approximately every
two weeks, until your
treatment is complete.
INVISALIGN
CONCLUSION
“The earlier treatmentbegins, the more the
face will adapt to your standards, the later
treatment begins the more your standards will
have to adapt to the face.”
C.Gugino
118.
REFERENCES
Orthodontics currentprinciples: 4th
edition- T.M.Graber
Hand book of orthodontics : 4th
edition - Moyers
Contemporary orthodontics : 4th
edition - Proffit
Dentistry for child and adolescent : 9th
edition - R.J.
McDonald
Textbook of orthodontics:2nd
edition- Gurkeerat singh
Orthodontics : 3rd
edition - SI.Balajhi
Functional appliances in orthodontic treatment- An atlas
of clinical prescription & lab construction. Harry S Orton
119.
Clinical Pedodontics: 4th
edition–Finn
Textbook of pedodontics:2nd
edition- Tandon
Occlusal guidance in pediatric dentistry – Nakata
Pediatric dentistry .infancy through adolescence: 4th
edition –
Pinkham
Google search
Myobrace.com
REFERENCES
#7 Hotz…bcos it implies tat knwldg of grwth n dev s necessary to drct the teeth as thy erpt into occlusn.
Lack of undrstndng n knwldg,it led to disastrous results
#8 DefineSerial extraction is a guided, progressive removal of deciduous teeth ahead of the time that they would normally be shed, “robbing Peter to pay Paul” to enlist the fundamental phenomena of adaptability and adjustment. By means of adaptability, providing room for certain teeth, there is an autonomous adjustment in the tooth position in Class I malocclusions. The technique is biologically sound, proven, and should not be considered a compromise. The objectives of establishing the integrity and proper position of the maxillary and mandibular incisors with the removal of deciduous canines are valid ones. The goal is to harmonize the defective tooth system with the normal muscle and bone systems in Class I malocclusions. The removal of deciduous first molars permits the early eruption of first premolars. If arch length is still obviously deficient, according to adequate diagnostic information available at that time, the first premolars are removed to allow the canine teeth to migrate distally into normal positions and to permit space closure by the mesial drift of the teeth posterior to the extraction site. In almost all instances, conventional orthodontic therapy is required to complete the alignment of teeth, to parallel the roots on either side of the extraction space, to eliminate overbite, and to effect residual space closure. However, such mechanotherapy is usually of significantly shorter duration, it is likely to produce less damage, and the results are more stable.
d the procedure refered to as serial extraction as the orderly removal of selected primary & permanent teeth in predetermined sequence
#18 B4 proceeding to the exn of certain deci teeth, Pri step is to assess tat a malocc exists on a clncl examntn nd need inv nd cllctn of diag rec.
SE bsd on thrgh diag nd crrid out carefully on slct grp of pts, procedur cn b excellnt and valuable trtmnt. Cn rduce applnc trtmnt tym,cost, discomfort to pt, and time lost by pt nd prnt
#23 A common xprsn , I may forget a name, but I’d neverforget a face.. Probably nothng fascinates a person more than the sight of another human face.. Human face is a living mirror held out to the world…
Color pictures are must - to record for future reference
the structure of enamel.
Add the dimension of color to the records- health of gingiva,
soft tissue.
#24 Stdy models prvide a 3 dimensional rec of the dentition an are essentil 4….
#30 .. allow spontaneous alignment of crowded incisors which simplify later appliance treatment.
.. accelerates the eruption of first premolar
…permanent canines to drift into natural alignment without any appliance.
#31 …has led to extraction of teeth in mixed dentition because the lips appear to be prominent.
…. is likely to cause a concave profile.
#34 One of the most crucial decisions tat the clinicians are req to make is whether to xtrct teeth for crctn of malocclusn.to do this, v need al d intllgnc, training and exprnc thy cn muster.
#37 To permit eruption & optimal alignment of lateral incisors.
Prevent maxillary lateral incisor in lingual cross bite.
Improvement in the position of central incisor.
#38 Permit canine to drift distally into the extracted space.
Earlier eruption of premolars
Slight improvement in anterior crowding
#39 The erupting premolar, once out of gingival margin is extracted.
If it is carried out correctly and if timing is right it is most exciting to see the bulging canine eminences move distally on their own into the premolar extraction sites.
This is more frequently seen in max than in man arch.
Modified dewel’s…..
#42 Mostly class I malocclusion , fall into this category. Most of the time , Rx procedure A is carried out. There are 8 groups in the class I whish requires serial xn. They are
#49 1.Shift from hard to soft diet.. Gen,,in mandi ant region..u/l presence leads to midline shift..interception by extraction would resolve malocclusion.
2. …impede eruptn of perm teethor erupt into malalignmnt.thrfr timly exn of d same wud go a long way in intrcp of dev MO.
Immd removal,obs and late removal.dpnds on size shape and nmbr.ideally, surg…does nt intrfr wth perm tooth dev
3.If c/l tooth fails to erupt evn aftr 3 mnths,thr shud b a concrn.surg intrvntn may b req.excision of fibrous oft tissues..or removl of any ovrlyng bone ovr d unerotd crwn s done. D soft or hard tissue excision s done in sch a way so as to xpose grtst dia of d unerptd tooth cwn or largr..ZOE drsng for 2 wks post surgiclly
4. Most common site is maxillary canine region..if the perm canine overlaps less than half of lat incisor root,thr s some hope of redirecting d canine distally smply by exn of pri canines.
#50 If pri canine exfoliates prematurely..midline shift..incisors tip lingually n dec arch length,,,it appear to b crrctd,bt only temp,,agn space shrtg s apparent wnh perm canines erpt..goal shud b to prvnt midline shift and manage space..
#51 Minimal resorption of pri molar, may b diffi to seat n also dislodge in an apical dirctn,..prio abscess..also nt radiopaque
If smll amt of mvmnt s needed..tightnd evry 2 wks..pdl space s cmprsd n molar s spaced distally until it can slip past d pri molar nd erupt
5. Metal button bonded to the occlsl srfc of impctd teeth…force of application or end of sprng drctly bonded to the teeth…bt salivry cntmntn of occlusl srfc..evaluated evry 2 wks..works effectively bcos of minimal root dev of 1st molar
Elastomeric chain changed monthly.
#52 Congenitally -premolar- substitute primary molar…ankylosis and root resorption…exn
If pri molars are ankylosed nr perm teeth missing..thn xtrct b4 vrtcl dscrpncy of the alveolus bcms too grt….implants or resto cn b placed and in sm cases space cn b clsd ortho
#53 Frst sign of crwdng in mxd dntition coincides wth eruptn of perm incisors.
50% resolution in perm dentition if physiologic spaces are bwn 2-3 mm,if 2 mm no intercptn wud b req.
No more than 4 mm..done on the mesial surfaces of deciduous canines followd by distal..if more space req thn mesial of deci 1st molars….topicl flride appl
Combi of obs and disking…..by many authors
Moderate crowding---expansion…headgears or lip bumper or elstomrc chains wth bonded brackets
Severe-crowdng >5mm..
3.Retaind deci teeth or sbmrgd teeth. Or extrac6t perm canines n lingual arch
4.Severe crwdng and dentoskeletal MO shud b referred
#54 No matter wt type of rx s used.. Retention s a prob and shud b plannd
If diastema reopens..frenectomy cn b perfrmd.. Evn aftr tat if reopens thn multistrnded wire bonded lingually..contraindi:deepbite n poor oral hygien
#55 Crrctn of dntl crsbyt in mxd dntitn s req bcos
#57 Tongue blade therapy/popsicle stick therapy-twenty times b4 each meal,pt counting to 5 each time,,,shud b done,several times at certain periods of d day….if nt successful within a week or 2,,other…….
Bite plane-steep enuf to giv a definite forward thrust;1/4th inch post..inclined plane s cut down and polished to propr angltn and height(2-3mm post bite opening) and tried and cemented…results wthn 2 wks.. 45degree to the long axis of lower inci..bite jumping wthn 1 week..
Doubl helical spring- acyivated 2 mm to provide 1 mm of tooth movmnt per month
With deep bite- open the bite by adding acrylic..crossbite wl crrct quickly nd biteplane cn b removd..extnded use creates vertical occlusal discrepancy
Post…are either gen or localised.. If b/l thn both of d abov.. If u/l thn unequal w arch or quads..
Crossbite elastics if u/l single tooth…elastic shud b worn until thr s slight overcorrection.. Leav the bands in place and discontinue the use of elastics for 1 month to ensure tat the teeth do not relapse into crossbite… nowadays buttons are availabl to bond directly to tooth.
W arch and quad helix-both dental and skeletal mvmnts…skeletal prb jack screw embedded in rmvbl applnc or shud b referd.
#59 The term ‘’myofunctional appliances’’and ‘’functional appliances’’,earlier on,have been used synonymously.Recent writings do not use the terms’’myofunctional’’at all.However,I would like to point out certain subtle differences between the two.
Myofunctional appliances are those appliances, which harness the muscle pressure to their advantage & thereby affect tooth movement.
Functional appliances are those appliances,which elicit certain natural functions of the orofacial region and thereby affect results.
#65 Certain myofunctional appliances have undergone so much use,study and research over the time that they themselves demand a
classification system viz.-Activator, Bionator, Frankel etc. A further dimension of active and passive appliances was incorporated and a new
system of classification advocated.
#67 Depth of sulcus
3, In case use for distooccl case constructn bite shd be aken to advance mand
Post extent last erupted molar
#71 The present form of app came through various stages of development starting with d concept of bite jumping introduced by kingsley
To be used in pt having retruded mand
This was folowed by hotz v. which is modfn of kingsley used in retro mand with deepbite
Single block of vulcanite,used in pts with glossoptosis and severe retrogntsm
He modified a Hawley type of retainer on the max arch for
which he added a lower horse-shoe shaped flange which
helped positioning the mandible forward.
#72 Acc to andr n haulp act induces musculosk adaptn by inducing a new pattern of mandibular closure
The patient has to move mandible forward to engage th appliance which results in stretching of elevator muscles of mastication.
This results in kinetic energy which: causes
Prevention forward growth of maxillary dento-alveolar process.
Distal movement of max dento-alveolar process.
Reciprocal forward force on mandible.
#74 Max n mand same as hawleys connect by interoccl part which makes this appl into a single block. Interocc part hav d intentatn of u n l teeth n caps d lower inc wic controls ther supraeruptn n proclinatn
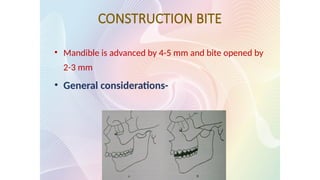
#75 It is an intermaxillary wax record used to relate the mandible to maxilla in dimensions of space, used to reposition the mandible in a forward directions well as opening the bite vertically.
Overjet too large- fwd positioning in 2-3 syages
Fed positioning of mand by 7-8mm the vertical opening shd b slight to mod 2-4mm
If fwd postin not more than 3-5mm then the vet openin can b 4-6mm
#76 Activator therapy aims at providing a good skeletal as well as dentoalveolar relationshipof u n l arches. Cant achieve simply by holding mand in fwd positn.to achieve proper 3 d relationship of teeth selective trimming is carried out
#77 Trimming is done to encourage the mesial movement of d lower molars n distal mov of upper therefore distopalatal surface of in max n mesiolingual surface in mand post seg r trimmed
#80 The bulkiness of d activator & its limitation to night time wear was amajor disadv .appl too bulky for day timt use
Moreover during night function is minimized or nonexistent.
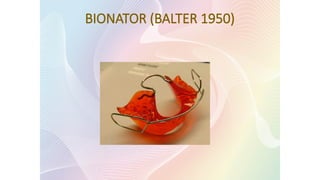
This led to dev of bionator a less bulky app. Its lower portion is narrow n its upre component has only lateral extension wit a cross palatal stabalizing bar.
Taking into cosideration the dominant role of the tongue posture balter designed app wic takes adv of tongue posture
#81 The equilibrium between the tongue & circumoral muscles is responsible for the shape of the arches & the functional space for the tongue are essential for the normal development of the orofacial systems
Moa-
The bionator doesn’t activate the muscles, but modulates the muscle activity thereby enhancing normal development of inherent growth pattern & eliminating the abnormal environmental factors.
#82 Causes sagital repositioning of mandible thereby increasing the oro functional space.
Causes anterior positioning of the tongue
prevents the external unfavorable muscle forces by means of vestibular arch and its buccal extension.
Intrusion and extrusion of teeth is obtained by loading or unloading the teeth with acrylic.
#83 Basic constructio
Class II div I having following features:
a. Well aligned dental arches
b. Retruded mandible
c. Mild skeletal discrepancy
d. Labial tipping of upper incisors
Class III malocclusion
Open bite cases
n same
#84 The appliance is constructed in such a way that:
The extension of the acrylic portion of the lower lingual part into the upper incisor region prevents thrusting of tongue between the anterior teeth which is responsible for causing open bite
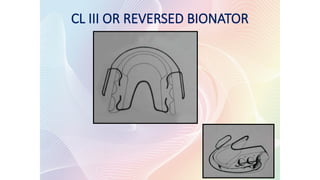
#85 Bite is taken in retruted position
Bite ia open by 2mm
Palatal bar configuration runs forward instead of posteriorly
#86 Frankel appliance holds the cheek and lip muscles away so the teeth have room to grow into the right position.
The Frankel appliance is designed to hold away the muscles (buccal and labial) from the dentition. So that the dento-alveolar structures are free to develop.
In addition, the Frankel appliance acts as an exercise device or an oral gymnastic device that aids in correction of the abnormal perioral muscle function.
#90 Frankel-III - CL-III malocclusion.
Here the lip pads are situated in the maxillary, instead of mandibular vestibular labial sulcus.
Labial bow rests against the mandibular teeth and not on the maxillary incisors.
There is a protrusive bow similar to that of Frankel-II behind the upper incisors to stimulate the forward movement of these teeth.
Effects: Frankel-III gives both skeletal & dental changes
Maxilla is moved in a forward & slightly downward direction.
(b) The mandible growth is redirected vertically with little evidence of antero-posterior repositioning of the chin.
#92 Cuspal inclined plane plays an important role in determining the relation of the teeth as they erupt into occlusion.
In case of class I relation the distal slope of the lower posterior teeth slide with the mesial slope of the upper posterior teeth creating a mesial component of force which is favourable for the normal mandibular development
In case of distoocclusion, the mesial slope of the lower posterior teeth slide with the distal slope of the upper posterior teeth creating a distal component of force that is unfavourable to normal forward mandibular development.
#93 The unfavourable cuspal contacts of the distal occlusion are replaced by favourable proprioceptive contact on the inclined plane of Twin block which frees the mandible from its locked distal functional position.
Due to the inclined plane effect a mesial component of force is created that is favourable for the normal development of mandible
#97 to apply a forward component of force to the upper arch and a downward and distal force to the mandible in the lower molar region.
#98 to apply a forward component of force to the upper arch and a downward and distal force to the mandible in the lower molar region.
#99 S p- aim is to maintsin incisor relationship until buccal segment occl is fully interdigited
Ret p- night time were of ant incl plane
#100 1st truelu fixed functional appliance developed by Emil Herbst (1900s).
Uses a telescopic mechanism & encourages forward repositioning
of the lower jaw as the patient closes into occlusion.
Pancherz 1982 & McNamara 1990 have shown that both skeletal and dental adaptations are produced with this appliance.
This was previously used in the mixed dentition period but now primarily used as an appliance in permanent dentition.
Artificail joint wrkng bwn the maxi n mandi..
#105 Such higher force produce hyalinization leading to undermining resorption,wic prevent tooth movement n thus only an orthopadic movement s seeen
2 acc to some author intermittent forces produce skeletal changes whereas continuous force produce dental movement
4,Mixed dentition period as it takes d adv of prepubertal growth spurts
5}inc in release of groth harmones more during the eve n night is assosiated with onset of sleep
#107 Commonly used orthopedic appliances
Used to intercept or correct skeletal malocclusion by distalising the maxillary dentition or maxilla it self.
#108 1 an in dis type is nape extn n distalizn of molars. Distal movement of maxilla
2. Distal translation of molars
3.Intrusion n distalizn
Distal n slightly superior force on max
#113
Mis system incorpoartes a near vertical pull headgear & its use in the management of
Encouraging an element of subsequent fwd
#114 LABIALY ant –incisal third
Occlusal coverage in the buccal seg does not extent onto the buccal surface of the premolar n molars
Even contact with mand dentition
Flying extraoral tractn tubes r incoperated which r alignedmesially to d cusp tip of 1st premolar
This allows the force frm d headgear to b tranferred to d appliance close to d considered center of resistance of the max dentitin which lies btn the premolar roots
Ant clasp can b incorp modified southend clap to minze palatal tipping
#115 Farell myofunctional research in australia usin g cad cam techniqueuo with silicone / non thermoplastic polyurethane produced myofunctional appliance company has come
The Pre-Orthodontic Trainer for Kids™ (T4K®) is a single size, prefabricated dental appliance that incorporates both myofunctional and tooth positioning characteristics. The T4K® is designed for treatment in the mixed dentition, while the permanent teeth are erupting and the child is still growing
#117 . Starting is a soft (Silicone) Phase 1 appliance and Finishing or Phase 2 is harder (Polyurethane).
#121 The BWS™ allows arch development and
anterior dental alignment to be combined without encroaching on the
natural position of the tongue. Therefore the force of the tongue can be
used in the treatment allowing the BWS™ to use very light force
The BENT WIRE System™ can be combined with fixed brackets and
the T4B™ (TRAINER for BRACES™) or T4CII™ allowing a seamless
integration from arch development, class II correction full fixed
brackets, while continuing the all important myofunctional training.
#122 The TRAINER System™ combined with the Farrell BENT WIRE
System™ are used for simultaneous arch development and treatment
of myofunctional habits. It can totally replace existing Phase I
treatment. This dual treatment approach gives substantial arch
development with very light forces from a simple and inexpensive
fixed appliance.
Advantages:
No palatal bar is needed, eliminating the speech and functional
problems of the common acrylic and quad helix appliances. The
aesthetic appeal of a completely lingual appliance and no speech
problems makes the BWS™ an easy favourite with patients. Because
the BWS™ is a fixed appliance, the compliance problems of phase
one-type appliances are eliminated. The patient enjoys normal speech
and no visible appliance during the day. As the BWS™ can also be
integrated with multi-banded appliances, it is a cost effective solution
to phase I treatment.
Stability is greatly improved due to the use of the TRAINER to
correct tongue position and function, plus mode of breathing. In fact
the technique depends on the use of the TRAINER System™ for its
effectiveness.
There’s no need for laboratory construction of the BWS™ - it can
#123 Wearing a Myobrace appliance for one to two hours each day and overnight while sleeping, combined with a series of 'myofunctional exercises' (also known as the Trainer Activities) each day is all that
uses light, intermittent forces to align the teeth. is required in the treatment process
The optimal patient age group is six to ten years of age
#124 Myobrace for Kids™ targets the underlying causes of crooked teeth as soon as the problems are evident, while the child's biological adaptability is at their peak. Improving these poor myofunctional habits at an early age allows for the child to have good dental alignment and improved jaw growth.
The Myobrace for Teens™ is a no-braces alternative to straightening teeth. Treatment involves using a series of removable orthodontic appliances combined with daily exercises to train the oral muscles and produce straighter teeth and a healthier smile.
The MYOBRACE for Adults™ works to align the teeth and correct the poor oral habits (also known as myofunctional habits) that are the real causes of crooked teeth and poor jaw growth. This process can straighten teeth without the need for complex retainers or braces.
#125
The i-3™ is prefabricated in small, medium and large-sized arch forms, eliminating the need for fitting or adjusting. The design is optimised for use in very early mixed dentition
From age 5-7
#126 Customisable Functional Appliance
T4F™ has the TRAINER attributes plus it can be moulded to fit tightly to the upper arch and locks in the mandible into Class I. Retains dental position and has the MYOFUNCTIONAL EFFECT™. The dual layer technology with moldable EVA outer skin is heated and fitted to the patient’s mouth. More bulky than the single larger TRAINERS, but the fit and retention are better. Replaces the need for laboratory made Class II activator or retainer.
Features:
Functional appliance, retainer after arch expansion, MYOFUNCTIONAL EFFECT™.
Dual layer, semi mouldable technology, thermoplastic outer material, for custom tight fit. Double Arch
Clinical Applications
Retainer after Class II correction, Interim Retainer Replacement for traditional “functional” appliances, retention between phase I and II treatment, Class II correction and retention. Early treatment with expansion or Class II correction can be lost while waiting for the permanent dentition.
More Information
Recommended minimum use – ONE HOUR DAILY plus OVERNIGHT WHILE SLEEPING
Thermoplastic outer material provides the convenience of "boil and bite" customised fit (regularly remouldable if adjustment is needed), Semi-rigid Polyurethane frame maintains shape and all design features during customization.
Customize in under 5 minutes - The T4F™ can be customised by fitting directly to the patient or indirectly using upper and lower models (preferred in mixed dentition).The T4F™ is heated in boiled water for 2 minutes then placed into the patient’s mouth after cooling for just one second under cold tap water. Position firmly into upper dentition then have the patient move the lower teeth into the bottom channel and bite down on the T4F™ as hard as possible. At the same time a vacuum is created by sucking in strongly with the lips closed and the tongue pushed up into the palate with the tip on the Tongue Tag. After holding this position for at least 20 seconds the T4F™ is removed and placed in cold water.
Class II correction AND myofunctional habit correction - Once customised, you have a Functional Appliance which is particularly good for Class II correction after maxillary expansion. As well as the Functional effect the T4F™ will also correct the associated myofunctional habits i.e. tongue thrusting, mouth breathing, a required feature missing from other commonly used orthopaedic appliances.
NO LAB FEES, no waiting, adjustable by remoulding - With the T4F™ there is no more waiting for lab construction. It can be fitted in the same time as it takes to make an impression and can be remoulded to accomodate erupting teeth or to improve the fit.
The T4F™ can be used to replace Class II correction "functional" appliances like the Clark Twin Block and Bionator. It is cheaper, easier to apply and will not break.
#127 Invisalign® takes a modern approach to straightening teeth, using a custom-made series of aligners created for you and only you. These aligner trays are made of smooth, comfortable and virtually invisible plastic that you wear over your teeth. Wearing the aligners will gradually and gently shift your teeth into place, based on the exact movements your dentist or orthodontist plans out for you. There are no metal brackets to attach and no wires to tighten. You just pop in a new set of aligners approximately every two weeks, until your treatment is complete. You’ll achieve a great smile with little interference in your daily life. The best part about the whole process is that most people won't even know you're straightening your teeth.
The aligners are easily removable, so you can continue to brush and floss your teeth as you normally would. Cleaning your aligners is just as easy with theInvisalign cleaning kit. Or you can simply brush and rinse them in lukewarm water. That's it! Achieving that great smile couldn't be easier!