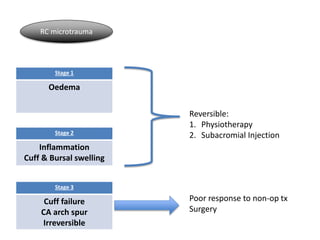
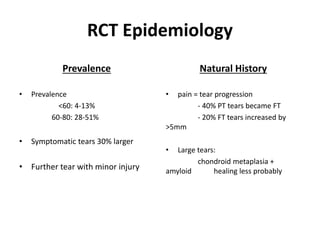
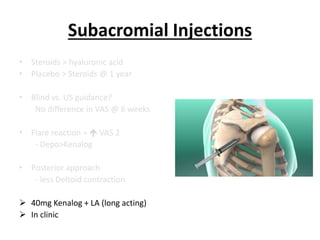
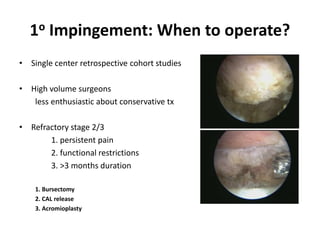
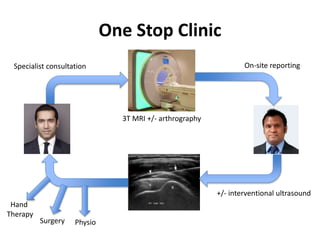
This document summarizes rotator cuff syndrome and arthroscopic subacromial decompression (ASAD). It discusses the anatomy and biomechanics of the rotator cuff. Common causes of rotator cuff pathology include impingement, tendinopathy, and tears. Conservative treatment includes physiotherapy and injections. ASAD is recommended for refractory stage 2 or 3 impingement, involving bursectomy, coracoacromial ligament release, and acromioplasty. Long-term studies show ASAD provides pain relief, improved function, and prevents future rotator cuff tears in the majority of patients. Patient selection, accurate diagnosis, and surgical technique affect outcomes.




![References
1. Neer CS 2nd. Anterior acromioplasty for the chronic impingement syndrome in the shoulder. 1972. J Bone
Joint Surg Am. 2005 Jun;87(6):1399.
2. Neer S 2nd. J Bone Joint Surg Am. Anterior acromioplasty for the chronic impingement syndrome in the
shoulder: a preliminary report. 1972 Jan;54(1):41-50.
3. Ellman H1, Kay SP. Arthroscopic subacromial decompression for chronic impingement. Two- to five-year
results. J Bone Joint Surg Br. 1991 May;73(3):395-8.
4. Ellman H1. Arthroscopic subacromial decompression: analysis of one- to three-year results. Arthroscopy.
1987;3(3):173-81.
5. Altchek DW1, Carson EW. Arthroscopic acromioplasty. Current status. Orthop Clin North Am. 1997
Apr;28(2):157-68.
6. Holmgren T1, Björnsson Hallgren H, Öberg B, Adolfsson L, Johansson K. Effect of specific exercise strategy on
need for surgery in patients with subacromial impingement syndrome: randomised controlled study. BMJ.
2012 Feb 20;344:e787. doi: 10.1136/bmj.e787.
7. Klintberg IH1, Svantesson U, Karlsson J. Long-term patient satisfaction and functional outcome 8-11 years
after subacromial decompression. Knee Surg Sports Traumatol Arthrosc. 2010 Mar;18(3):394-403. doi:
10.1007/s00167-009-0963-1. Epub 2009 Oct 23.
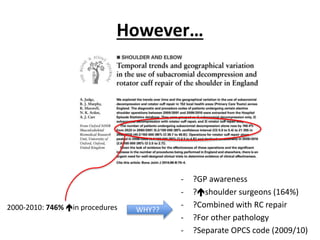
8. Judge A1, Murphy RJ, Maxwell R, Arden NK, Carr AJ. Temporal trends and geographical variation in the use of
subacromial decompression and rotator cuff repair of the shoulder in England. Bone Joint J. 2014 Jan;96-
B(1):70-4. doi: 10.1302/0301-620X.96B1.32556.
9. Speer KP1, Lohnes J, Garrett WE Jr. Arthroscopic subacromial decompression: results in advanced
impingement syndrome. Arthroscopy. 1991;7(3):291-6.
10. Hawkins RJ1, Plancher KD, Saddemi SR, Brezenoff LS, Moor JT. Arthroscopic subacromial decompression. J
Shoulder Elbow Surg. 2001 May-Jun;10(3):225-30.
11. Bouchard A1, Garret J2, Favard L3, Charles H4, Ollat D5. Failed subacromial decompression. Risk factors.
Orthop Traumatol Surg Res. 2014 Dec;100(8 Suppl):S365-9. doi: 10.1016/j.otsr.2014.09.006. Epub 2014 Oct
29.
12. Odenbring S1, Wagner P, Atroshi I. Long-term outcomes of arthroscopic acromioplasty for chronic shoulder
impingement syndrome: a prospective cohort study with a minimum of 12 years' follow-up. Arthroscopy.
2008 Oct;24(10):1092-8. doi: 10.1016/j.arthro.2008.04.073. Epub 2008 Jun 16.
13. Klintberg IH1, Svantesson U, Karlsson J. Long-term patient satisfaction and functional outcome 8-11 years
after subacromial decompression. Knee Surg Sports Traumatol Arthrosc. 2010 Mar;18(3):394-403. doi:
10.1007/s00167-009-0963-1. Epub 2009 Oct 23.
14. Björnsson H1, Norlin R, Knutsson A, Adolfsson L. Fewer rotator cuff tears fifteen years after arthroscopic
subacromial decompression. J Shoulder Elbow Surg. 2010 Jan;19(1):111-5. doi: 10.1016/j.jse.2009.04.014.
15. Arcand MA1, O'Rourke P, Zeman CA, Burkhead WZ Jr. Revision surgery after failed subacromial
decompression. Int Orthop. 2000;24(2):61-4.
16. Kappe T1, Knappe K, Elsharkawi M, Reichel H, Cakir B. Predictive value of preoperative clinical examination
for subacromial decompression in impingement syndrome. Knee Surg Sports Traumatol Arthrosc. 2013 Jan
22. [Epub ahead of print]
17. Lim JT1, Acornley A, Dodenhoff RM. Recovery after arthroscopic subacromial decompression: prognostic
value of the subacromial injection test. Arthroscopy. 2005 Jun;21(6):680-3.
18. Singh HP1, Mehta SS2, Pandey R2. A preoperative scoring system to select patients for arthroscopic
subacromial decompression. J Shoulder Elbow Surg. 2014 Sep;23(9):1251-6. doi: 10.1016/j.jse.2014.05.030.
19. Ogilvie-Harris DJ1, Wiley AM, Sattarian J. Failed acromioplasty for impingement syndrome. J
Bone Joint Surg Br. 1990 Nov;72(6):1070-2.
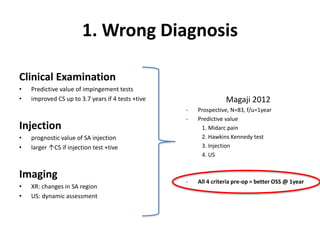
20. Magaji SA1, Singh HP, Pandey RK. Arthroscopic subacromial decompression is effective in selected patients
with shoulder impingement syndrome. J Bone Joint Surg Br. 2012 Aug;94(8):1086-9. doi: 10.1302/0301-
620X.94B8.29001.
21. Dopirak R1, Ryu RK. Management of the failed arthroscopic subacromial decompression: causation and
treatment. Sports Med Arthrosc. 2010 Sep;18(3):207-12. doi: 10.1097/JSA.0b013e3181eb6ce8.
22. Gartsman GM1, O'connor DP. Arthroscopic rotator cuff repair with and without arthroscopic subacromial
decompression: a prospective, randomized study of one-year outcomes. J Shoulder Elbow Surg. 2004 Jul-
Aug;13(4):424-6.
23. Massoud SN, Levy O, Copeland SA. Subacromial decompression. Treatment for small- and medium-sized tears
of the rotator cuff. J Bone Joint Surg Br. 2002 Sep;84(7):955-60.
24. Weinstein DM1, Bucchieri JS, Pollock RG, Flatow EL, Bigliani LU. Arthroscopic debridement of the shoulder for
osteoarthritis. Arthroscopy. 2000 Jul-Aug;16(5):471-6.
25. Guyette TM1, Bae H, Warren RF, Craig E, Wickiewicz TL. Results of arthroscopic subacromial decompression
in patients with subacromial impingement and glenohumeral degenerative joint disease. J Shoulder Elbow
Surg. 2002 Jul-Aug;11(4):299-304.
26. Hutchinson MR1, Veenstra MA. Arthroscopic decompression of shoulder impingement secondary to Os
acromiale. Arthroscopy. 1993;9(1):28-32.
27. Wright RW1, Heller MA, Quick DC, Buss DD. Arthroscopic decompression for impingement syndrome
secondary to an unstable os acromiale. Arthroscopy. 2000 Sep;16(6):595-9.
28. Youm T1, Hommen JP, Ong BC, Chen AL, Shin C. Os acromiale: evaluation and treatment. Am J Orthop (Belle
Mead NJ). 2005 Jun;34(6):277-83.
29. Marder RA1, Heiden EA, Kim S. Calcific tendonitis of the shoulder: is subacromial decompression in
combination with removal of the calcific deposit beneficial? J Shoulder Elbow Surg. 2011 Sep;20(6):955-60.
doi: 10.1016/j.jse.2010.10.038. Epub 2011 Feb 1.
30. Balke M1, Bielefeld R, Schmidt C, Dedy N, Liem D. Calcifying tendinitis of the shoulder: midterm results after
arthroscopic treatment. Am J Sports Med. 2012 Mar;40(3):657-61. doi: 10.1177/0363546511430202. Epub
2011 Dec 8.
31. Tillander BM1, Norlin RO. Change of calcifications after arthroscopic subacromial decompression. J Shoulder
Elbow Surg. 1998 May-Jun;7(3):213-7.
32. Fischer BW1, Gross RM, McCarthy JA, Arroyo JS. Incidence of acromioclavicular joint complications after
arthroscopic subacromial decompression. Arthroscopy. 1999 Apr;15(3):241-8.
33. Barber FA1. Coplaning of the acromioclavicular joint. Arthroscopy. 2001 Nov-Dec;17(9):913-7.
34. Kharrazi FD1, Busfield BT, Khorshad DS. Acromioclavicular joint reoperation after arthroscopic subacromial
decompression with and without concomitant acromioclavicular surgery. Arthroscopy. 2007 Aug;23(8):804-8.
35. Soyer J1, Vaz S, Pries P, Clarac JP. The relationship between clinical outcomes and the amount of arthroscopic
acromial resection. Arthroscopy. 2003 Jan;19(1):34-9.
36. Donigan JA1, Wolf BR. Arthroscopic subacromial decompression: acromioplasty versus bursectomy alone--
does it really matter? A systematic review. Iowa Orthop J. 2011;31:121-6.
37. Güven Z1. Rehabilitation following anterior acromioplastyActa Orthop Traumatol Turc. 2003;37 Suppl 1:119-
27.
38. Hultenheim Klintberg I1, Gunnarsson AC, Styf J, Karlsson J. Early activation or a more protective regime after
arthroscopic subacromial decompression--a description of clinical changes with two different physiotherapy
treatment protocols--a prospective, randomized pilot study with a two-year follow-up. Clin Rehabil. 2008 Oct-
Nov;22(10-11):951-65. doi: 10.1177/0269215508090771.](https://image.slidesharecdn.com/rotatorcuffsyndromeiseh1-171119221435/85/Rotator-cuff-syndrome-49-320.jpg)































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)




