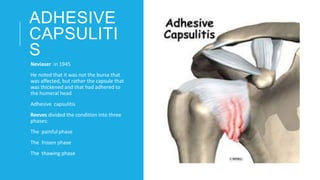
Adhesive capsulitis, also known as frozen shoulder, is characterized by substantial restriction of both active and passive shoulder motion in the absence of a known shoulder disorder. It most commonly affects individuals aged 40-60 years old and is more prevalent in females. The condition involves three phases - a painful phase with nagging shoulder pain that worsens at night, a freezing phase with progressive stiffness and loss of shoulder movement, and a resolution phase with gradual improvement in range of motion. Clinical presentation includes pain, restricted range of motion especially in external rotation, and weakness from disuse. Potential causes include extended immobilization, mild trauma, diabetes, and other medical conditions.