













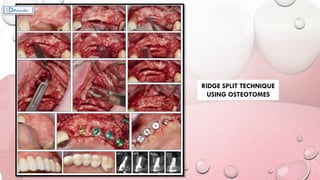

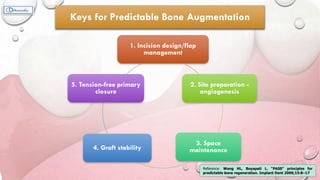

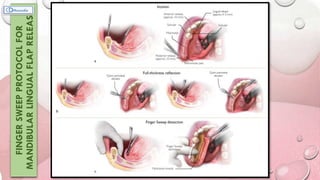

















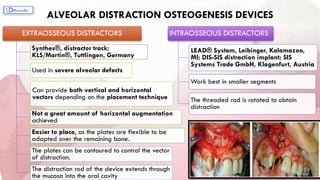






This document provides information on various ridge augmentation techniques. It begins with an introduction describing how tooth loss leads to bone resorption and impaired function. It then discusses the history of using autogenous bone grafts for ridge augmentation. The objectives of ridge augmentation are also outlined. Key techniques discussed include ridge preservation, ridge splitting, use of autogenous bone blocks, and distraction osteogenesis. Advantages and disadvantages of different graft sources and incision designs are compared. The document emphasizes the importance of adequate bone volume for successful implant placement and summarizes various methods to augment bone.























































































