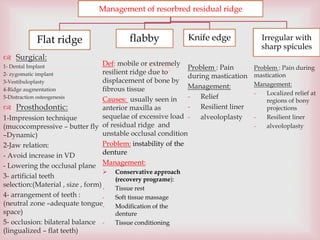
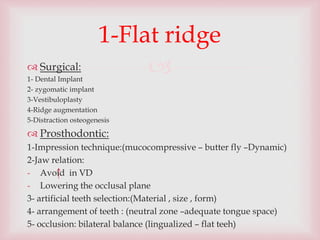
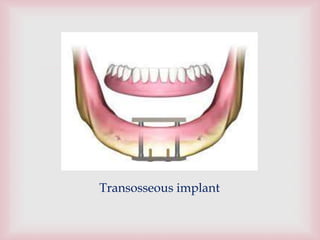
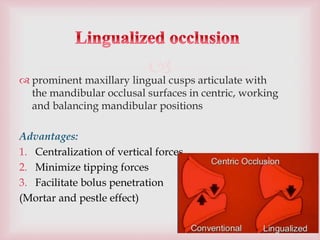
This document discusses the management of residual ridges after tooth loss. It covers various types of residual ridges including flat, flabby, knife edge, and irregular ridges with sharp bony spicules. For each ridge type, both surgical and prosthodontic management approaches are described. Surgical options include dental implants, vestibuloplasty, ridge augmentation, and distraction osteogenesis. Prosthodontic options focus on impression techniques, jaw relation records, tooth selection and arrangement, and providing balanced occlusion. The document emphasizes preserving remaining tissues, maintaining proper vertical dimension and occlusal plane, and distributing forces to reduce ridge resorption.