1) Applied respiratory physiology examines the links between basic respiration and clinical manifestations of respiratory diseases, including respiratory adjustments to health stresses, disturbances of respiration, artificial respiration, and pulmonary function tests.
2) Disturbances of respiration include abnormal respiratory patterns like tachypnea and apnea, as well as issues related to respiratory gases and pulmonary diseases.
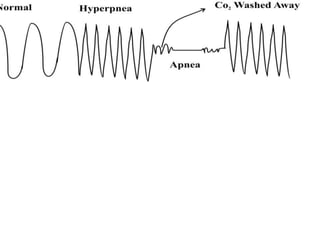
3) Specific abnormal respiratory patterns discussed include eupnea, tachypnea, bradypnea, polypnea, apnea, hypoventilation, hyperventilation, hyperpnea, and dyspnea.