Downloaded 1,066 times
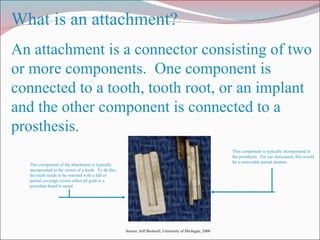
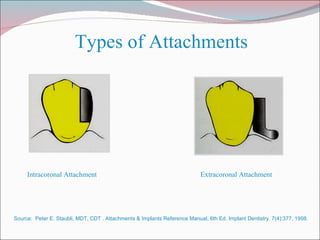


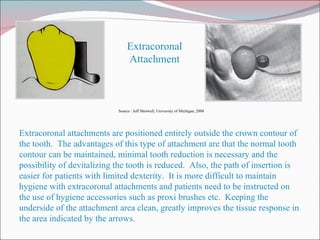



1. An attachment is a connector used in removable partial denture fabrication that connects a component fixed to a tooth to a component incorporated into the denture prosthesis. 2. There are two main types of attachments: intracoronal attachments contained within the crown and extracoronal attachments positioned outside the crown. 3. Attachments require the restoration of abutment teeth with crowns and involve the incorporation of male and female attachment components into the crowns and denture respectively.



































































