

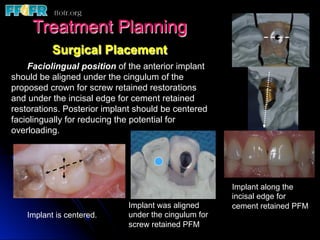
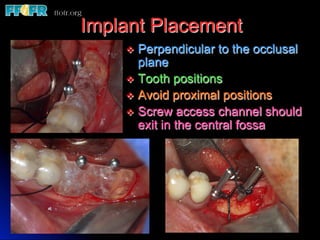
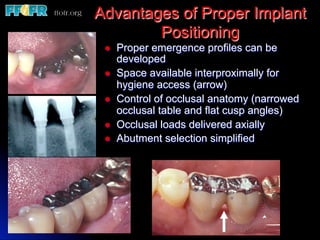
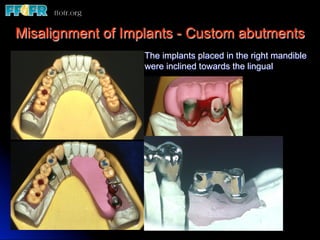
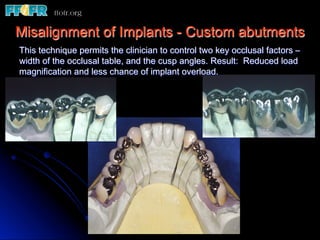




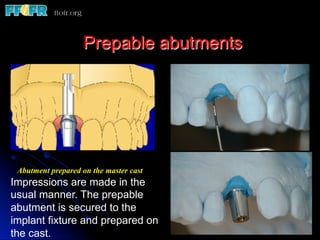

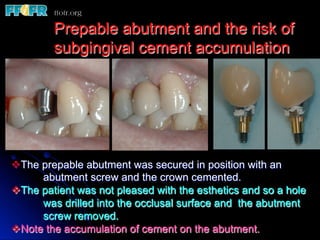
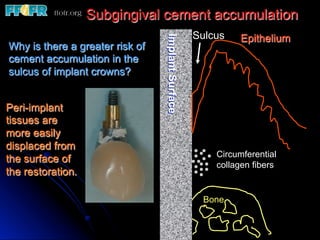
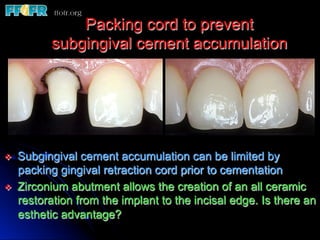
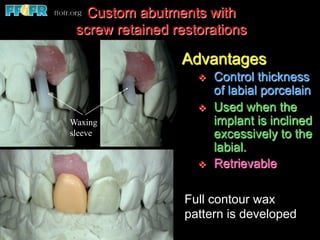
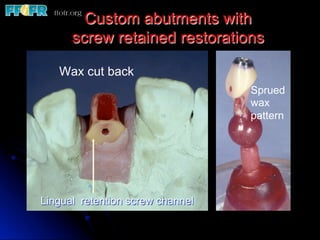

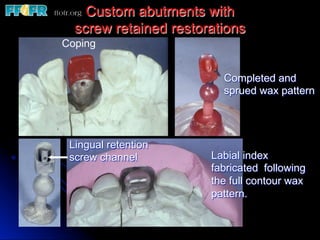



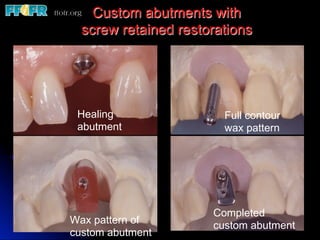



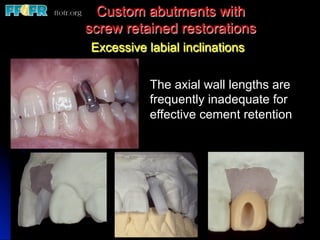



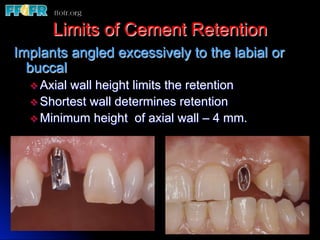
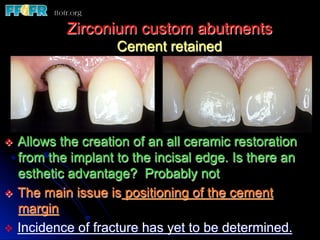
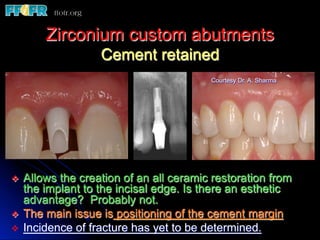

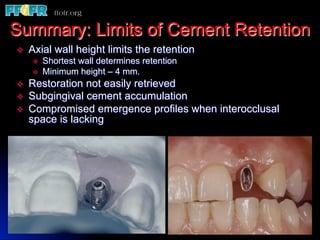


This document discusses various options for connecting dental restorations to implants, including screw retained, cement retained, and screwless systems. It highlights advantages and disadvantages of different abutment selections and placement positions. Custom abutments are described as an option to control porcelain thickness and manage excessive implant inclinations, though excessive angulation can compromise cement retention. Packing retraction cord and lingual access holes are presented as ways to reduce the risk of subgingival cement accumulation.

























![Prosthodontic management of endodontically treated teeth [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/prosthodonticmanagementofendodonticallytreatedteethautosaved-210611115147-thumbnail.jpg?width=640&height=640&fit=bounds)





























































