
More Related Content
Similar to Spots for Biochemistry
Similar to Spots for Biochemistry (20)
More from RAJNKIT
More from RAJNKIT (14)
Recently uploaded
Recently uploaded (20)
Spots for Biochemistry
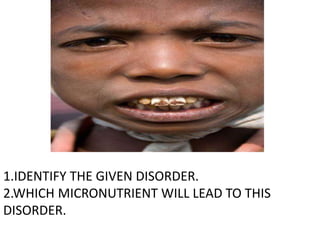
- 1. 1.IDENTIFY THE GIVEN DISORDER. 2.WHICH MICRONUTRIENT WILL LEAD TO THIS DISORDER.
- 2. 1.IDENTIFY THE GIVEN DISORDER. 2.WHICH MICRONUTRIENT WILL LEAD TO THIS DISORDER.
- 3. 1.IDENTIFY THE GIVEN DISORDER. 2.WHICH MICRONUTRIENT WILL LEAD TO THIS DISORDER. 3.WRITE TWO BIOCHEMICAL PARAMETERS WHICH GETS ALTERED IN THIS DISORDER. 4.WHICH AGE GROUP GETS AFFECTED BY THIS DISORDER.
- 4. 1. IDENTIFY THE GIVEN DISORDER. 2.WRITE TWO BIOCHEMICAL PARAMETERS ALTERED IN THIS DISORDER.
- 5. 1. IDENTIFY THE GIVEN DISORDER. 2. WRITE TWO BIOCHEMICAL PARAMETERS ALTERED IN THIS DISORDER.
- 6. 1. IDENTIFY THE GIVEN DISORDER. 2.WRITE TWO BIOCHEMICAL PARAMETERS ALTERED IN THIS DISORDER. 3.WHICH MICRONUTRIENT WILL LEAD TO THIS DISORDER. 4.WHICH AGE GROUP GETS AFFECTED BY THIS DISORDER.
- 7. 1.IDENTIFY THE GIVEN DISORDER. 2.WRITE THE BIOCHEMICAL PARAMETERS ALTERED IN THIS DISORDER.
- 8. Serum Bilirubin (Total) Conjugated Bilirubin Unconjugated Bilirubin SGOT (AST) SGPT (ALT) Alkaline phosphatase Hb 5.0 mg/dL 4.5 mg/dL 0.5 mg/dL 38 IU/L 36 IU/L 856 IU/L 12 gm % Urine Bilirubin Bile salts Urobilinogen +++ +++ - -- Stool Stercobilinogen --- Patient came to surgical OPD with complaints of pain abdomen, itching all over the body and passing clay colored stools. Results of biochemical tests are as follows:- 1. Identify the most probable type of jaundice. 2. What may be the cause which may lead to above jaundice.
- 9. Serum Bilirubin (Total) Conjugated Bilirubin Unconjugated Bilirubin SGOT (AST) SGPT (ALT) Alkaline phosphatase Hb 5.0 mg/dL 3.0 mg/dL 2.0 mg/dL 200 IU/L 280 IU/L 123 IU/L 12 gm % Urine Bilirubin Bile salts Urobilinogen + + present Stool Stercobilinogen --- A young male came with complaints of nausea, vomiting and lose of Appetite, malaria, fever and pain in right upper abdomen. Results for the Biochemical tests are as follows:- 1. Identify the most probable type of jaundice. 2. What may be the cause which may lead to above jaundice.
- 10. Serum Bilirubin (Total) Conjugated Bilirubin Unconjugated Bilirubin SGOT (AST) SGPT (ALT) Alkaline phosphatase Hb 5.0 mg/dL 0.5 mg/dL 4.5 mg/dL 38 IU/L 36 IU/L 123 IU/L 7.2 gm % Urine Bilirubin Bile salts Urobilinogen --- --- +++ Stool Stercobilinogen +++ A patient reported OPD with complain of passing reddish colored urine . On examination yellow discoloration of sclera was seen. Results for biochemical tests were as follows:- 1. Identify the most probable type of jaundice. 2. What may be the cause which may lead to above jaundice
- 11. A 37 yrs old individual was brought to the emergency room in a state of shock. He also had a low urine output. His renal function is shown as under : Serum urea – 210 mg/dL Serum creatinine – 2.0mg/dL 1.What is the normal blood urea level? 2.What kind of kidney disease is this?
- 12. The value of serum glucose was given as 360 mg/dL by a clinical laboratory. Convert this value into mmol/L [MW. of glucose 180]
- 13. Calculate creatinine clearance from the following values:- Plasma Creatinine – 1.0mg/dl Urine Creatinine – 60mg/dL Volume of urine – 2400ml/day
- 14. A young patient reported to the O.P.D by his parents with the complaint that he has mental retardation. A tendency for hypo pigmentation of skin associated with eczema was observed. Provisionally the case was diagnosed as a PKU (Phenylketonuria). 1. Suggest laboratory investigation to confirm the diagnose. 2. What is the reason for hypopigmentation?
- 15. A 15 years old boy was brought in a state of coma to the hospital. Onset of condition was sudden. He was having a deep and heavy kind of breathing. He also had a fruity odor in his breath. Blood glucose done at the time revealed a level of 825mg/dL.Benedict’s and Rothera’s test were positive. 1. What is the probable clinical diagnosis? 2.What is the basis of the fruity odour in his breath?
- 16. A 5 years old child was brought to the hospital with mental retardation and frequent episodes of hypoglycemia. On examination the child was also detected having cataract. Urine examination of the child showed presence of reducing substances. He was diagnosed to be a case of Galactosemia. However the blood glucose was low. 1. Which enzyme deficiency results in the above condition? 2. Why did the child have cataract?
- 17. Patient was investigated and blood urea was reported as 150 mg/dl. 1.Mention three conditions in which blood urea increases 2.Calculate blood urea nitrogen (BUN) for the above value.
- 18. 1. Identify the plot. 2.What is the type of inhibition seen and justify the answer. [1/V] [1/S] Inhibitor No inhibitor
- 19. 1. Identify the plot. 2. What is the type of inhibition seen and justify the answer. No Inhibitor [1/V] [1/S] Inhibitor
- 20. 60 year old man was brought to the emergency department with severe chest pain radiating towards the left shoulder with breathlessness, vomiting and profuse sweating. The clinician on duty suspected myocardial infarction (MI). 1.Which enzyme assay is most diagnostic in this case? 2.What is the earliest biochemical marker to diagnose MI?
- 21. PARAMETERS NORMAL RANGE pH 7.35 – 7.45 pCO2 35 - 45 HCO3 22 - 26 pH pCO2 HCO3 7.30 36 18 Interpret the ABG report of a given patient. 1. Identify the abnormality. 2. Justify your answer.
- 22. PARAMETERS NORMAL RANGE pH 7.35 – 7.45 pCO2 35 - 45 HCO3 22 - 26 Interpret the ABG report of a given patient pH pCO2 H CO3 7.28 56 25 1. Identify the abnormality. 2.Justify your answer.
- 23. PARAMETERS NORMAL RANGE pH 7.35 – 7.45 pCO2 35 - 45 HCO3 22 - 26 Interpret the ABG report of a given patient. pH pCO2 HCO3 7.53 36 30 1. Identify the abnormality. 2.Justify your answer.
- 24. A boy aged 5 yrs was brought to the hospital with abdominal swelling. On examination the liver was found to be enlarged. Biochemical tests showed increased uric acid, FFA, and hypoglycemia.The boy was diagnosed with Von Gierke’s disease. 1.Hypoglycemia was due to …. 2.Name another manifestation (sign/ symptom) of this disease.
- 25. A 50 yr old man with a history of spontaneous fractures and deep aching pains which are aggravated by carrying weights. On investigation levels of calcium , phosphorous and alkaline phosphate were raised. 1.What are the normal levels of serum alkaline phosphate ? 2.Write 2 physiological states in which alkaline phosphate is raised.
- 26. Q1) Identify the disease which causes periorificial and acral dermatitis In infancy and children due to zinc deficiency Q2) Give its recommended alloted reuirement.
- 27. History of photosensitivity, pain abdomen,Nausea vomiting,anxiety Cutaneous blisters darkening of skin ,Rashes, On sun exposure, high colored urine,Mental confusion , seizures Q1) Identify the disease? Q2) Tests in urine?
- 28. History of weakness , tiredness, paleness On examination... Palor, glossitis , koilonychia (spoon shaped nails), cheilitis Q1)Which condition is it? Q2) What is the recommended daily alloted requirement?
- 29. Patient presents with night blindness, white spots on cornea , clear part of cornea becomes cloudy and softens... Keratomalacia Spiny keratenous papules On elbow and forearm.. Phrynoderma Q1)Which vit deficiency? Q2)Recommend daily allotted requirement? Q3)Source: ?
- 30. Bruising, bleeding gums, weakness, fatigue and rash. Petichae Q1)Name the disease? Q2)Name the deficient vitamin? Q3)Recommended daily allotted requirement? And source?
- 31. Mutation in gene for copper transport protein Kinky hair (Sparse hair),growth failure, nervous system deterioration Symptoms develop in infancy,do not live past 3 years Q1) Identify the disease Q2) Which mineral is deficeint.
- 32. Rash on the face, lips, feet, or hands. In some people, dermatitis forms around the neck, a symptom known as Casal necklace. Other Symptoms include inflamed skin, diarrhea, dementia, and sores in the mouth. Q1)Identify disease? Q2)Which vitamin defeciency? Q3)Source ?
- 33. Lipid storage disease characterized by deposition of glucosecerebroside in cells of macrophage monocyte system .Enlarge liver and sprain, low number of RBCs (Anemia),easy bruising due to decreased blood platelets. Q1)Name the Disease Q2) Which enzyme deficiency?
- 34. A group of metabolic disorders caused by the absence or malfunctioning of lysosomal enzymes needed to break down molecules called glycosaminoglycans(GAGs). These long chains of sugar carbohydrates occur within the cells that help build bone, cartilage, tendons, corneas, skinand connective tissue. GAGs (formerly called mucopolysaccharides) are also found in the fluid that lubricate joints There is abnormal accumulation of heparan sulfate, dermatan sulfate, and keratan sulfate. Q1) Identify the group of the metabolic disorders. Q2) Give two examples.
- 35. Q. 1 Identify the disease ? Q.2 What is accumulated ? • Patients with disease are unable to degrade phytanic acid because of a deficient activity of phytanoyl-CoA hydroxylase (PhyH), a peroxisomal enzyme catalyzing the first step of phytanic acid alpha-oxidation. • It is an autosomal recessive trait • There is complex developmental sequelae, and progressive disabilities. • Peripheral polyneuropathy, cerebellar ataxia, , retinits pigmentosa and ichthyosis are the major clinical components. The symptoms evolve slowly and insidiously from childhood through adolescence and early adulthood. • Symptoms begin by late childhood or adolescence, although there are reports of presentation as late as 50 years of age. • Disease presents with anosmia and early-onset retinitis pigmentosa, with variable neuropathy, deafness, ataxia and ichthyosis. • Treatment • Phytanic acid is obtained from the diet, particularly from meat and dairy products. Dietary restriction helps to control sensory neuropathy, myopathy, ataxia and ichthyosis. In acute presentation