Downloaded 37 times








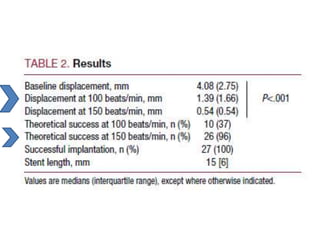
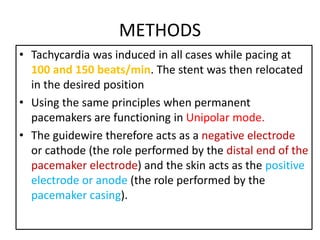
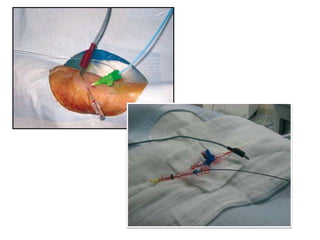



This document discusses techniques to stabilize coronary stents before deployment during percutaneous coronary intervention (PCI). It describes several methods commonly used such as deep guide catheter engagement, anchoring wires, and temporary pacing. The floating wire technique is highlighted as being well-suited for right coronary artery lesions due to the weaker backup support of Judkins catheters in that vessel. Induced tachycardia using temporary pacing is described as an effective alternative to right ventricular pacing that avoids central venous access. Limitations of different techniques are also reviewed.














































































